1. Burn Tissue Injury
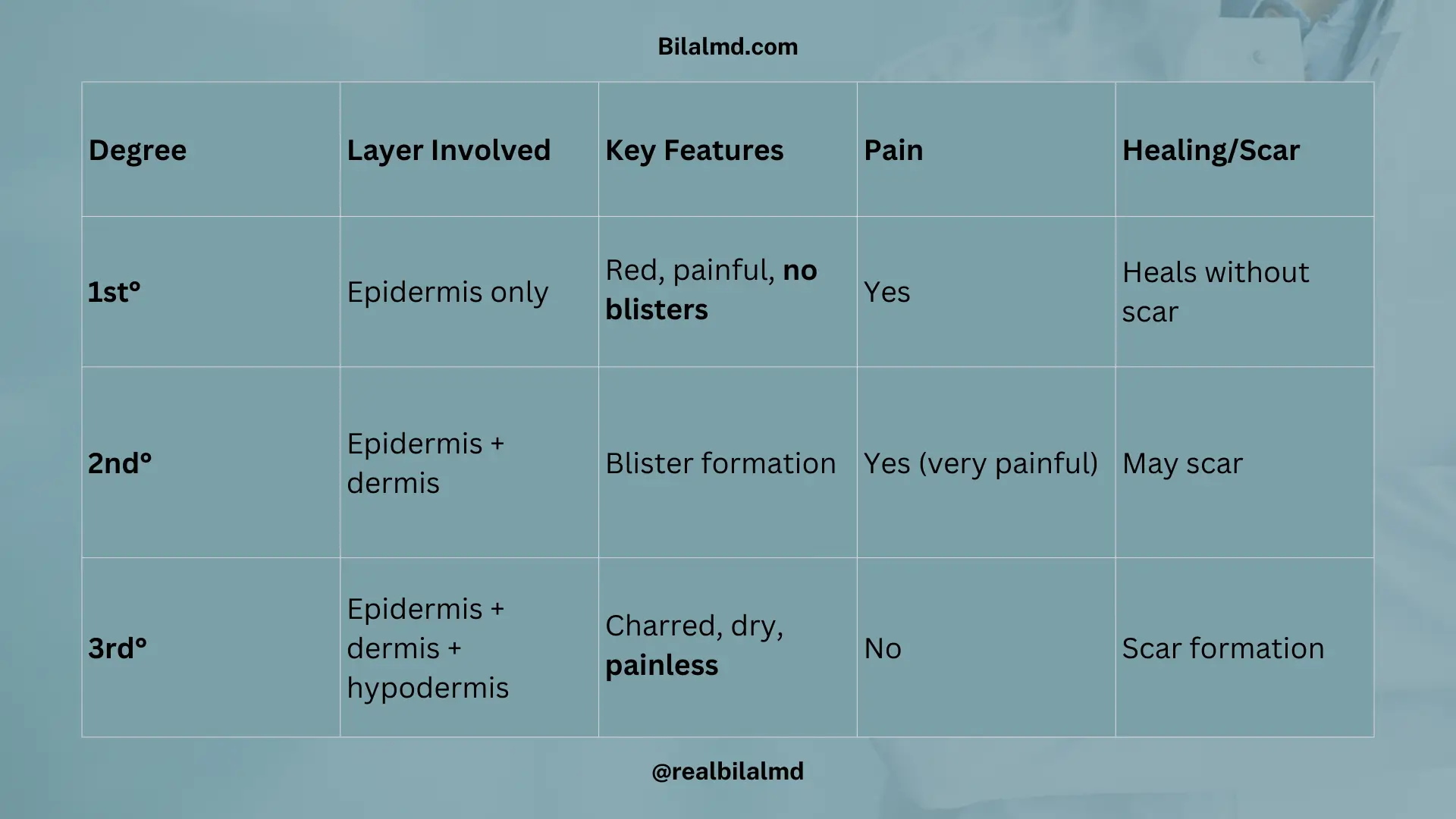
1. Types
- 1st degree → Epidermis only (red, painful, no blister)
- 2nd degree → Epidermis + dermis → blister formation
- 3rd degree → Epidermis + dermis + hypodermis (subcutaneous tissue) → painless, scar formation
2. Common Infection
- Pseudomonas aeruginosa
3. Fluid Resuscitation
Parkland Formula Fluid (ml)=4[Weight (kg)×%BSA(burned)]
- Half in the first 8 hours
- The remaining half in the next 16 hours
🔹 Example:
Weight = 70 kg, Burn area = 5% BSA
4×70×5=1400 ml
Here are other materials for NLE NRE step 1
2. Shock
Mnemonic for shock types → SHOCk
- S: Septic
- H: Hypovolemic
- O: Obstructive
- C: Cardiogenic
1. Hypovolemic Shock
- Cause: ↓ blood/fluid volume
- Dehydration
- Diarrhea
- Burns
- Hemorrhage
- First sign → Tachycardia
- Peripheral signs → Cold, clammy extremities
- Treatment:
- IV fluids (crystalloids)
- Blood transfusion (if hemorrhage)
2. Obstructive Shock
- Cause: Mechanical obstruction to filling/emptying of the heart
- Cardiac tamponade
- Tension pneumothorax
- Massive pulmonary embolism
- Mechanism → Heart can’t relax/fill properly
- Treatment → Relieve obstruction (pericardiocentesis, chest tube, thrombolysis)
3. Cardiogenic Shock
- Cause: Pump failure (heart cannot contract effectively)
- Myocardial infarction (MC cause)
- Cardiomyopathy
- Severe valvular disease
- Signs → Cold periphery, hypotension, pulmonary edema
- Treatment → Inotropes (dobutamine), revascularization
4. Distributive Shock
Mechanism: Severe vasodilation → maldistribution of blood → warm periphery
(a) Anaphylactic Shock
- Type I Hypersensitivity (IgE mediated → histamine release → vasodilation, edema, bronchospasm)
- Treatment: Adrenaline IM (1:1000, 0.3–0.5 mg), airway support, antihistamines, steroids
(b) Septic Shock
- Cause: Infection (often gram-negative bacteria → endotoxin release)
- Signs:
- Vasodilation + warm periphery
- Hypotension
- High-grade fever
- Treatment:
- Norepinephrine (α1 agonist) = DOC
- Broad-spectrum antibiotics
- IV fluids
(c) Neurogenic Shock
- Cause: Spinal cord injury (above T6) → ↓ sympathetic tone, ↑ parasympathetic tone → vasodilation + bradycardia
- Signs: Warm, dry skin + hypotension + bradycardia
- Treatment: Treat underlying cause, vasopressors, atropine if severe bradycardia
Cold periphery → Hypovolemic, Cardiogenic, Obstructive
Warm periphery → Septic, Anaphylactic, Neurogenic
| Type | Cause | Mechanism | Clinical Signs | Treatment |
|---|---|---|---|---|
| Hypovolemic | Hemorrhage, dehydration, diarrhea, burns | ↓ Intravascular volume → ↓ preload → ↓ CO | Early tachycardia, hypotension, cold clammy skin | IV crystalloids, blood transfusion |
| Obstructive | Cardiac tamponade, tension pneumothorax, massive PE | Physical obstruction → impaired filling/output | Hypotension, JVP ↑ (tamponade), muffled HS, pulsus paradoxus | Relieve obstruction (pericardiocentesis, chest tube, thrombolysis) |
| Cardiogenic | MI, cardiomyopathy, valvular disease, arrhythmias | Pump failure → ↓ CO despite normal volume | Hypotension, cold clammy periphery, pulmonary edema | Inotropes (dobutamine), revascularization, diuretics |
| Distributive – Anaphylactic | Drugs, food, insect bite (IgE-mediated) | Histamine release → vasodilation + ↑ permeability | Warm skin, flushing, edema, bronchospasm | Adrenaline IM, airway, antihistamines, steroids |
| Distributive – Septic | Gram -ve bacteria (endotoxin), sepsis | Cytokines → vasodilation + capillary leak | Warm periphery, hypotension, fever, tachycardia | Norepinephrine, IV fluids, broad-spectrum antibiotics |
| Distributive – Neurogenic | Spinal cord injury (T6↑), anesthesia | Loss of sympathetic tone → vasodilation + bradycardia | Warm, dry skin, hypotension, bradycardia | Vasopressors, atropine, treat cause |
3. Abnormal Scars
| Type | Definition | Key Features |
|---|---|---|
| Hypertrophic scar | Excess collagen (Type I & III) within original wound boundary | Raised, red scar, but does not extend beyond wound |
| Keloid | Excess collagen (mostly Type III) extends beyond wound margin | Irregular, hard, itchy, common in ear lobes, chest, shoulders, darker skin |
Key Difference:
- Keloid = Beyond the boundary
- Hypertrophic = Within boundary
3. Wound Healing & Scar Formation
| Type | Definition (as per your info) |
|---|---|
| Primary intention | Original wound margins are approximated and closed with stitches. |
| Secondary intention | Wound left open → granulation tissue forms → later replaced with scar. |
| Delayed (Tertiary) intention | Wound healing delayed due to recurrent infection. |
4. Indirect vs Direct Inguinal Hernia
| Feature | Indirect Hernia | Direct Hernia |
|---|---|---|
| Pathway | Herniated organ enters through deep inguinal ring → exits via superficial inguinal ring | Hernia pierces fascia directly |
| Structure involved | Passes through transversalis fascia | Weakness of fascia (direct bulge) |
| Age group | Young age | Older age |
| Bulge test | No bulge (+Ve test) | Bulge present (+Ve test) |
| Relation to Inferior Epigastric Artery | Lateral to inferior epigastric artery | Medial to inferior epigastric artery |
5. Scrotal Complaints
| Condition | Key Feature | Prehn’s Sign | Transillumination | Special Note / Exam Finding | Treatment |
|---|---|---|---|---|---|
| Testicular torsion | Sudden pain, tender, high-riding testis | Negative (pain not relieved) | – | Surgical emergency | Urgent surgery |
| Epididymitis | Gradual pain, fever, tender epididymis | Positive (pain relieved) | – | Often post-infective | Antibiotics |
| Varicocele | Left-sided, venous retention, “bag of worms” | –ve | – | More prominent on standing/Valsalva | Surgery if symptomatic/infertility |
| Hydrocele | Scrotal swelling, smooth, fluctuant | –ve | Positive (transmits light) | Examiner can get above swelling | Surgery if persistent |
| Inguinoscrotal hernia | Scrotal swelling, expansile cough impulse | –ve | Negative | Cannot get above swelling | Surgery |
Key clinical points:
- Cannot get above swelling → Hernia.
- Prehn’s sign + → Epididymitis (infection).
- Prehn’s sign – → Torsion (emergency).
- Transillumination + → Hydrocele.
- Bag of worms → Varicocele.
6. Neck Lump
| Type / Duration | Key Features | Location / Notes | Treatment |
|---|---|---|---|
| < 3 weeks | Inflammatory lymph node | Usually tender, red, swollen | Treat underlying infection (lymphadenitis) |
| > 3 weeks | Alarming sign → investigate further | Could be cyst or tumor | Depends on underlying cause |
| Dermoid cyst | Congenital cyst | Midline, usually upper/middle neck | Surgical excision |
| Sebaceous cyst | Acquired, contains keratin/sebum | Dermal | Drainage or excision |
| Lipoma | Painless lump, fatty tissue | Anywhere on neck | Observation or excision if large |
| Painful lumps | Dermoid disease, influenced by hormones (↑F, ↓estrogen) | – | Surgical if symptomatic |
| Hashimoto / Thyroiditis | Neck mass | Thyroid region | Manage thyroid condition |
| Thyroglossal cyst | Midline neck mass, moves with swallowing or tongue protrusion | Midline | Surgical excision (Sistrunk procedure) |
| Ectopic thyroid | Sublingual mass | Under tongue | Depends on thyroid function, may require surgery |

7. Thyroid Malignancy
| Type | Age / Risk Factors | Origin | Spread / Metastasis | Key Findings / Markers | Prognosis |
|---|---|---|---|---|---|
| Papillary Ca | Any age; ↑ risk with childhood radiation | Follicular cells | Lymphatic route | Psammoma bodies, Orphan Annie nuclei | Good |
| Follicular Ca | 40–60 yrs | Follicular cells | Hematogenous | – | Early detection → good; late detection → poor |
| Medullary Ca | – | Parafollicular (C cells) | – | Calcitonin tumor marker; Tetany; associated with MEN 2A, MEN 2B | – |
| Anaplastic Ca | >60 yrs | Poorly differentiated | – | Rare, aggressive | Poor prognosis |
8. Thyroid Nodule & Scan
| Feature | Details |
|---|---|
| Hot Nodule | ↑ Radioactive iodine uptake |
| Cold Nodule | ↓ Radioactive iodine uptake; 20% malignant → FNAC / biopsy required |
9. Post-Thyroid Surgery Complications
| Complication | Cause / Details |
|---|---|
| Hematoma | Can compress the airway → open the stitch immediately |
| Hoarseness of voice | Recurrent laryngeal nerve (RLN) damage |
| Bleeding control | Ligate the middle thyroid vein |
| Hypocalcemia | Parathyroid gland removed → ↓ calcium |
10. Breast Cancer
| Feature | Details / Notes |
|---|---|
| Gender | F > M |
| Common Location | Upper outer quadrant |
| Risk Factors | Advanced age, Family history (BRCA1, BRCA2), Estrogen exposure (nulliparity), Alcohol intake, HER2 mutation |
| Alarming Signs | Breast asymmetry, Skin dimpling, Nipple discharge, Palpable lump |
| Treatment / Targeted Therapy | Doc: Trastuzumab (HER2 positive) |
| Other Notes | Fat necrosis: history of trauma → necrosis; Mastitis: lump + fever, chills, rigor |

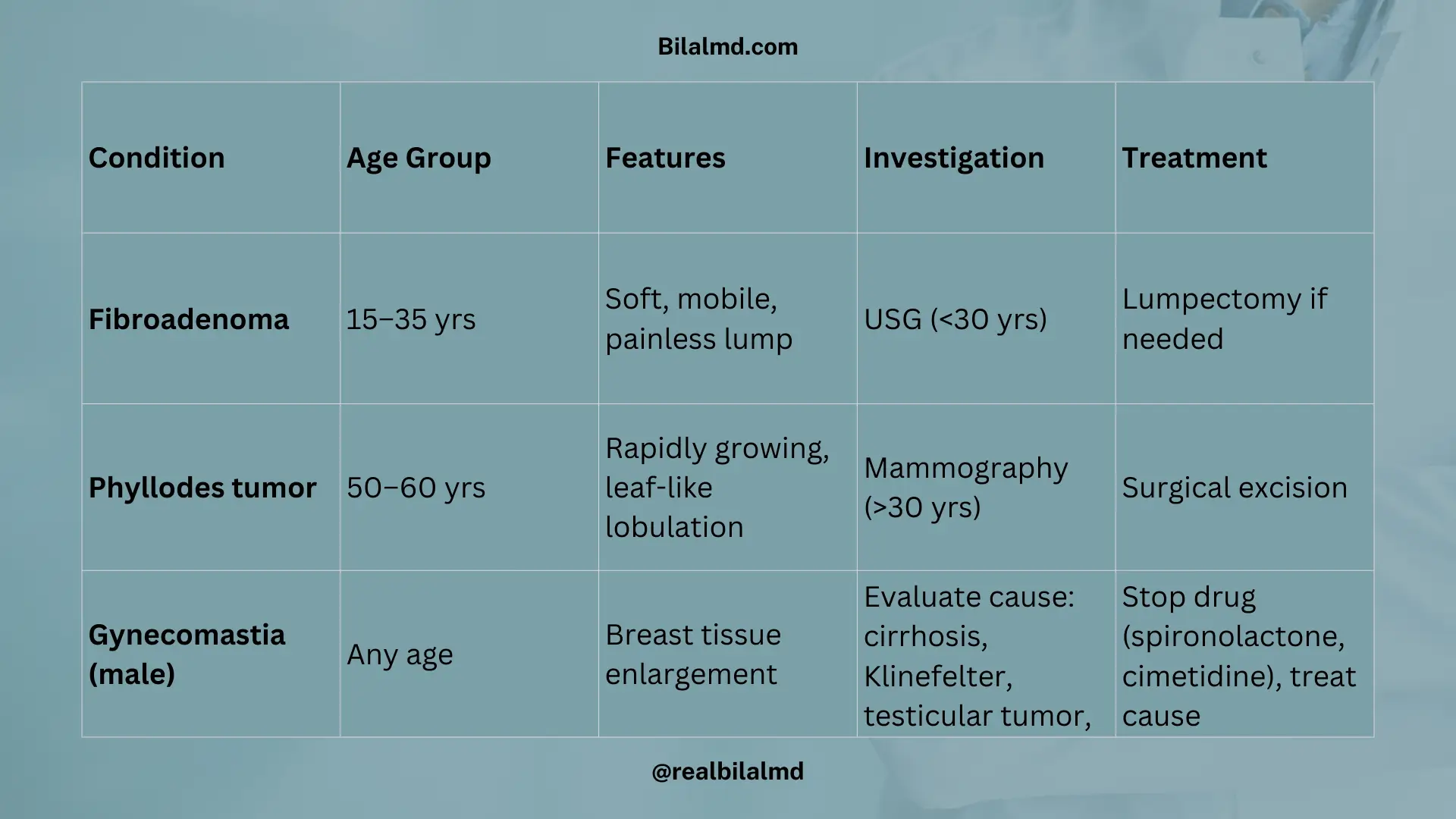
11. Benign Breast Conditions
| Condition | Age Group | Features / Notes | Investigation | Treatment |
|---|---|---|---|---|
| Fibroadenoma | 15–35 yrs | Soft, painless, mobile lump | USG <30 yrs | Lumpectomy if needed |
| Phyllodes tumor | 50–60 yrs | Breast lump, size increasing, leaf-like lobulation | Mammography >30 yrs | Surgical excision |
| Gynecomastia (male) | Any adult male | Enlargement of breast tissue | – | Evaluate underlying cause: cirrhosis, Klinefelter (47XXY), testicular tumor, Tx. (spironolactone, cimetidine) |
Check your NRE Step 1 result after completing the exam.