1. Gout
- Cause: Increased serum uric acid → deposition of monosodium urate (MSU) crystals in joints.
- Common Site:
- 1st MTP joint (great toe) → Podagra.
- Subcutaneous tissue → Tophi.
- Lab Findings:
- Serum uric acid (S. UA) > 7.5 mg/dL.
- Joint aspiration → Needle-shaped, negatively birefringent crystals (under polarized light).
- Clinical Features:
- Acute: Joint pain, swelling, redness, tenderness.
- Treatment:
- Acute attack: NSAIDs (first-line).
- Chronic management:
- Allopurinol (xanthine oxidase inhibitor).
- Febuxostat (alternative; side effect = diarrhea).
- Drug Interaction:
- Allopurinol + Azathioprine → Severe bone marrow suppression.
2. Pseudogout
- Cause: Deposition of calcium pyrophosphate crystals.
- Lab Findings:
- Joint aspiration → Rhomboid-shaped, positively birefringent crystals.
| Feature | Gout | Pseudogout |
|---|---|---|
| Crystal type | Monosodium urate (MSU) | Calcium pyrophosphate (CPPD) |
| Crystal shape | Needle-shaped | Rhomboid-shaped |
| Birefringence | Negative birefringence | Positive birefringence |
| Common site | 1st MTP joint (Podagra) | Knee joint (most common) |
| Subcutaneous deposit | Tophi | Rare |
| Serum finding | ↑ Uric acid (>7.5 mg/dL) | Normal uric acid |
| Acute treatment | NSAIDs | NSAIDs, Colchicine |
| Chronic treatment | Allopurinol, Febuxostat | Non-specific (manage underlying cause) |

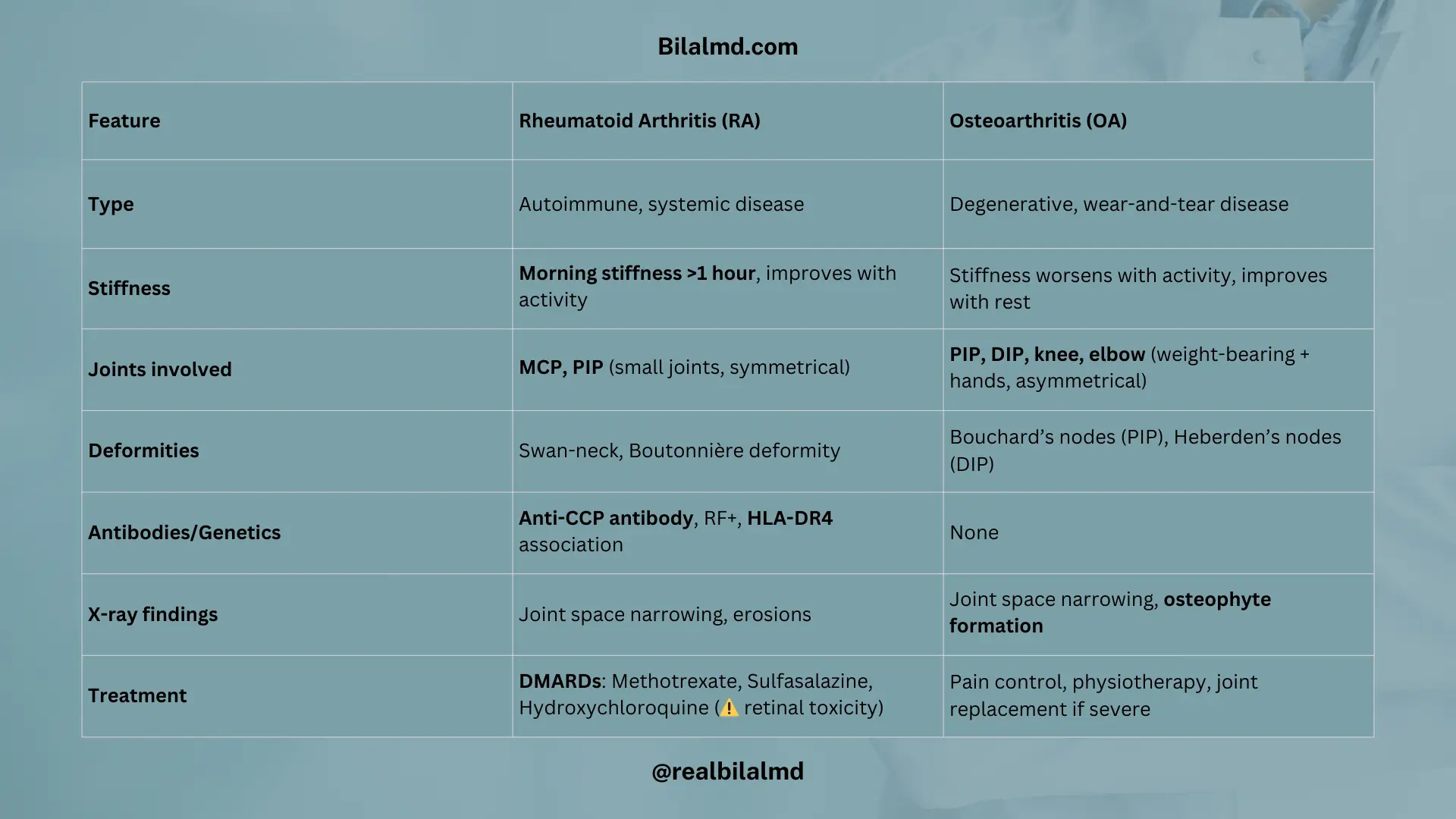
3. Rheumatoid Arthritis (RA) vs Osteoarthritis (OA)
| Feature | Rheumatoid Arthritis (RA) | Osteoarthritis (OA) |
|---|---|---|
| Type | Autoimmune, systemic disease | Degenerative, wear-and-tear disease |
| Stiffness | Morning stiffness >1 hour, improves with activity | Stiffness worsens with activity, improves with rest |
| Joints involved | MCP, PIP (small joints, symmetrical) | PIP, DIP, knee, elbow (weight-bearing + hands, asymmetrical) |
| Deformities | Swan-neck, Boutonnière deformity | Bouchard’s nodes (PIP), Heberden’s nodes (DIP) |
| Antibodies/Genetics | Anti-CCP antibody, RF+, HLA-DR4 association | None |
| X-ray findings | Joint space narrowing, erosions | Joint space narrowing, osteophyte formation |
| Treatment | DMARDs: Methotrexate, Sulfasalazine, Hydroxychloroquine (⚠️ retinal toxicity) | Pain control, physiotherapy, and joint replacement if severe |
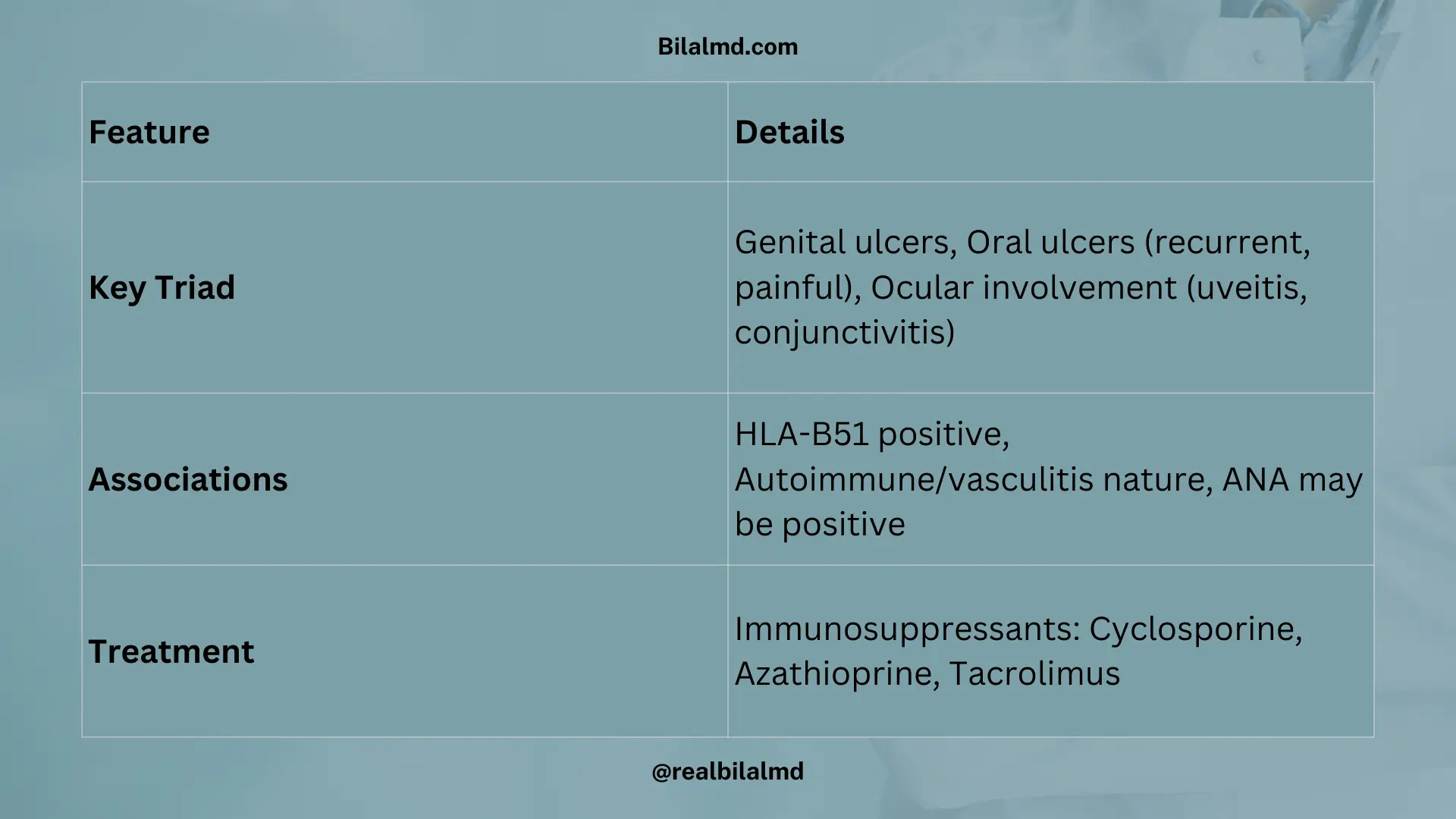
4. Behcet’s Syndrome
Key Features (Triad)
- Genital ulcers
- Oral ulcers (recurrent, painful)
- Ocular involvement (uveitis, conjunctivitis)
Associations
- HLA-B51 positive (strong genetic link)
- Autoimmune/vasculitis nature
- ANA may be positive (non-specific)
Treatment
- Immunosuppressants:
- Cyclosporine
- Azathioprine
- Tacrolimus
Here are other materials for NLE NRE step 1
5. Felty’s Syndrome
- Triad:
- Rheumatoid Arthritis (RA)
- Splenomegaly
- Neutropenia
6. Caplan’s Syndrome
- Seen in patients with Rheumatoid Arthritis (RA) + pneumoconiosis.
- Characterized by:
- Lung nodules (multiple, round).
- Associated with occupational dust exposure (e.g., coal workers).
7. Septic Arthritis
Definition
Inflammation of a joint due to bacterial infection.
Common Causes
- Staphylococcus aureus (most common)
- Gram-negative rods (e.g., E. coli, Pseudomonas)
Clinical Features
- Severe joint pain
- High-grade fever, chills, rigors
- Redness, swelling, and tenderness of the affected joint
Investigations
- Joint aspiration (gold standard)
- ↑ WBC count (>80,000/mm³)
- Gram stain & culture → identifies organism
- Blood tests → leukocytosis, ↑ ESR/CRP
Treatment
- Empiric antibiotics:
- Ceftriaxone + Vancomycin (cover Gram+ and Gram–)
- Drainage of joint fluid (arthrocentesis or surgical washout)
- Modify antibiotics according to culture results
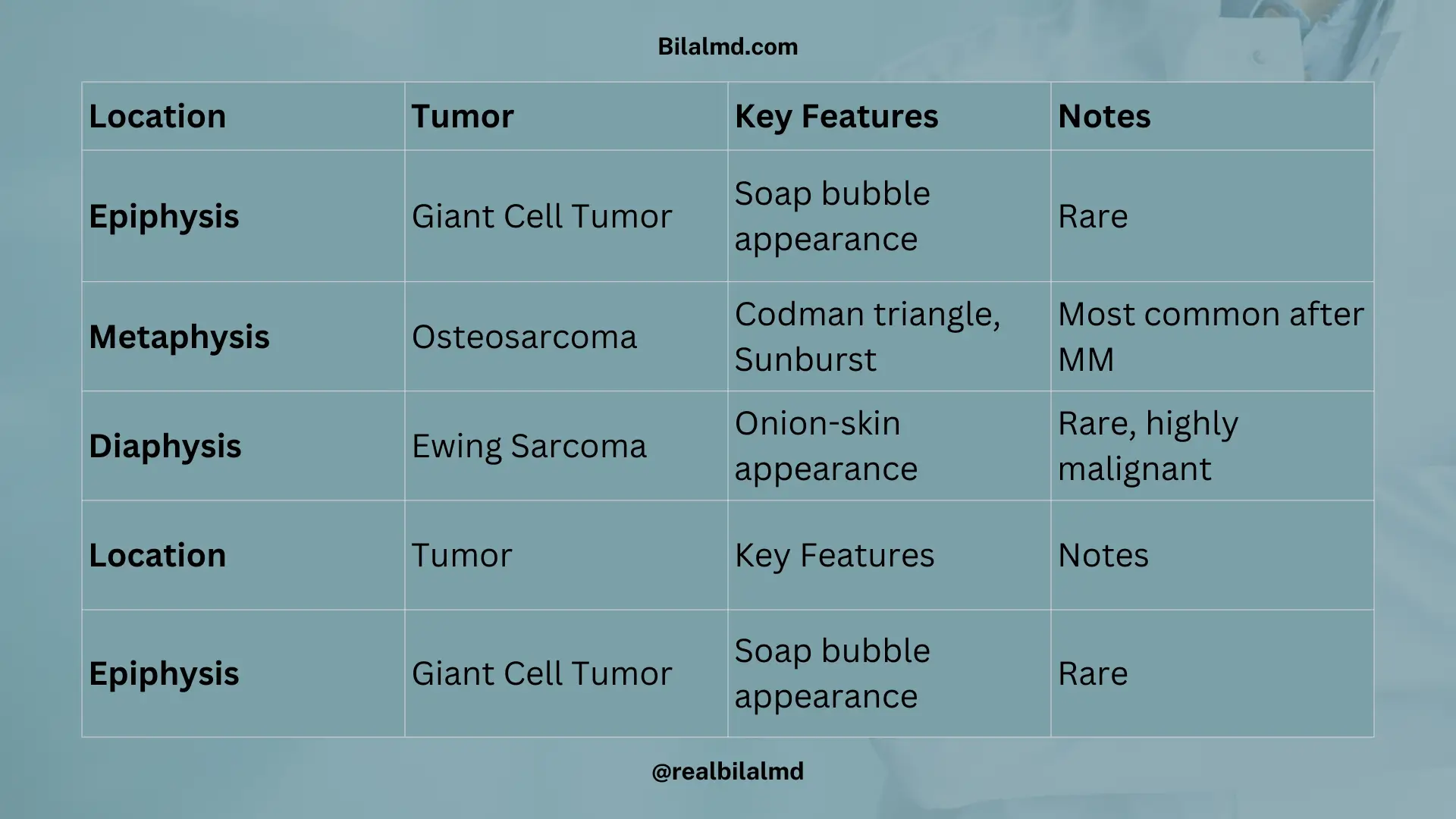
8. Bone Tumors – Quick Review
- E = Epiphysis → Giant cell tumor
- D = Diaphysis → Ewing sarcoma
- M = Metaphysis → Osteosarcoma
| Location | Tumor | Key Features | Notes |
|---|---|---|---|
| Epiphysis | Giant Cell Tumor | “Soap bubble” appearance on X-ray | Rare |
| Metaphysis | Osteosarcoma | Most common primary bone tumor (after MM) | Codman triangle, sunburst |
| Diaphysis | Ewing Sarcoma | “Onion-skin” / “Onion ring” appearance | Rare, highly malignant |
9. Osteosarcoma
- Age: 10–20 years
- Weight: 40–60 kg
- X-ray:
- Sunburst appearance
- Codman’s triangle
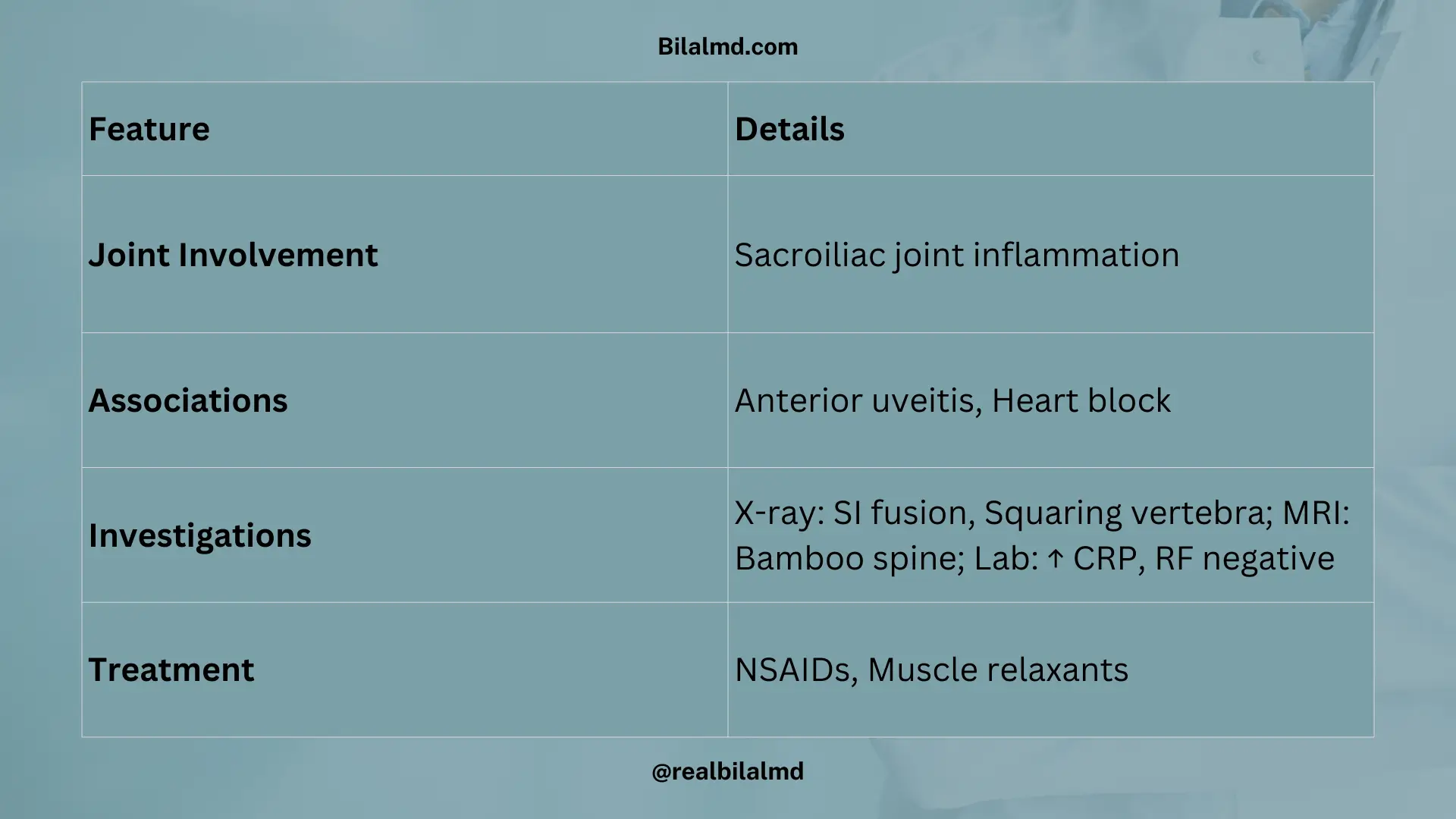
10. Seronegative Arthritis – Ankylosing Spondylitis
- Joint Involvement: Inflammation of the sacroiliac joint
- Associations:
- Anterior uveitis
- Heart block
- Investigations:
- X-ray: Fusion of the sacroiliac joint, squaring of the lumbar vertebrae
- MRI: Bamboo spine
- Lab: ↑ CRP, Rheumatoid factor (–ve)
- Treatment:
- NSAIDs
- Muscle relaxants
11. Reactive Arthritis (Reiter’s Syndrome)
- Triad:
- Conjunctivitis
- Arthritis
- Urethritis
12. Psoriatic Arthritis
- Joint involvement: Commonly, DIP joints
- X-ray: Pencil-in-cup deformity
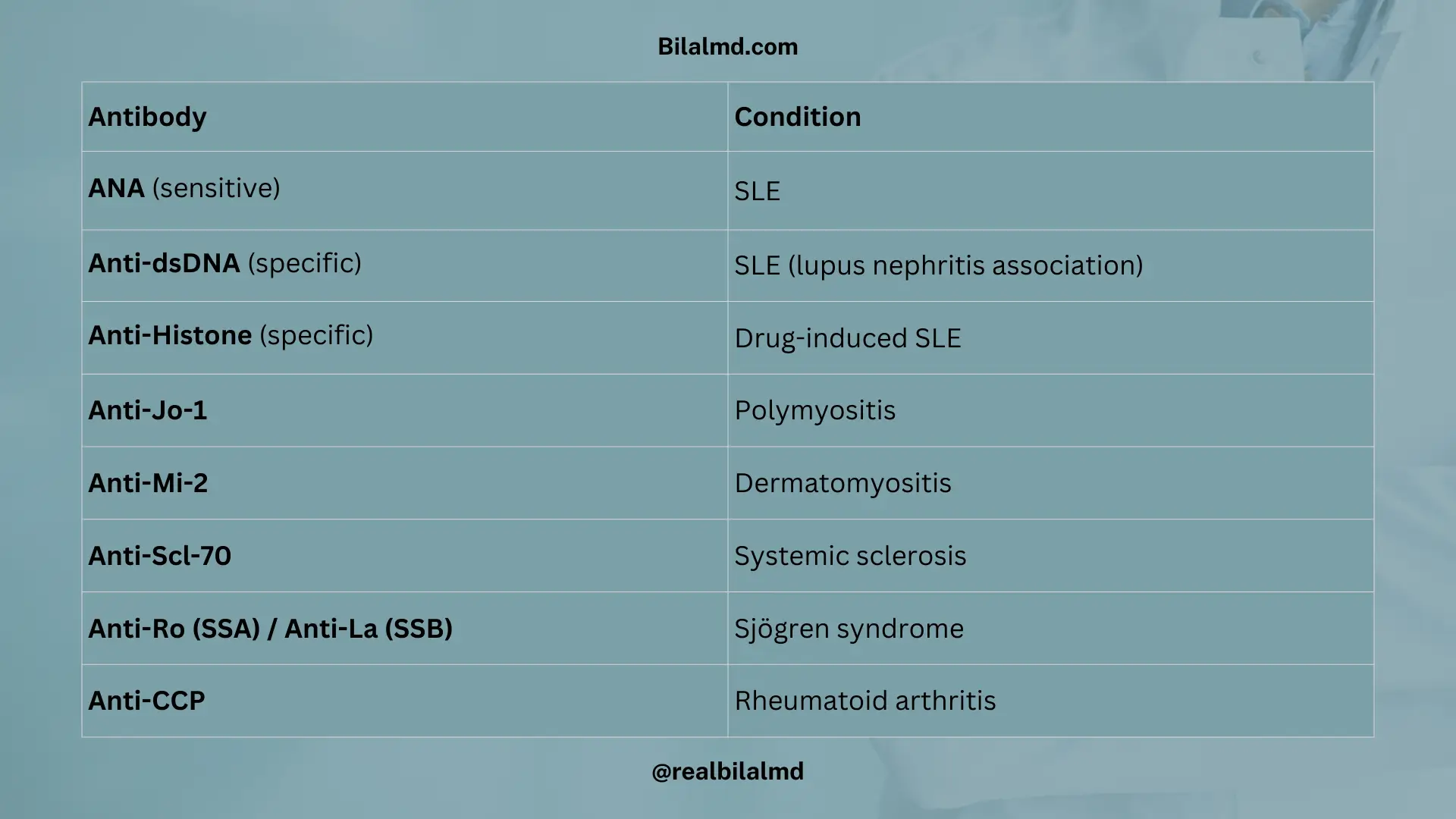
13. Important Antibodies & Their Associated Conditions
| Antibody | Condition |
|---|---|
| ANA (sensitive) | SLE |
| Anti-dsDNA (specific) | SLE (lupus nephritis association) |
| Anti-Histone (specific) | Drug-induced SLE |
| Anti-Jo-1 | Polymyositis |
| Anti-Mi-2 | Dermatomyositis |
| Anti-Scl-70 | Systemic sclerosis |
| Anti-Ro (SSA) / Anti-La (SSB) | Sjögren syndrome |
| Anti-CCP | Rheumatoid arthritis |
14. Polymyositis
- Meaning: Poly = many, myositis = muscle inflamed
- Clinical feature:
- Progressive muscle weakness (esp. proximal muscles → difficulty standing, climbing stairs, combing hair)
- No skin involvement (distinguishes from dermatomyositis)
- Antibody: Anti-Jo-1 antibody
- Diagnosis: Muscle biopsy (gold standard)
- Treatment: Steroids (first-line)
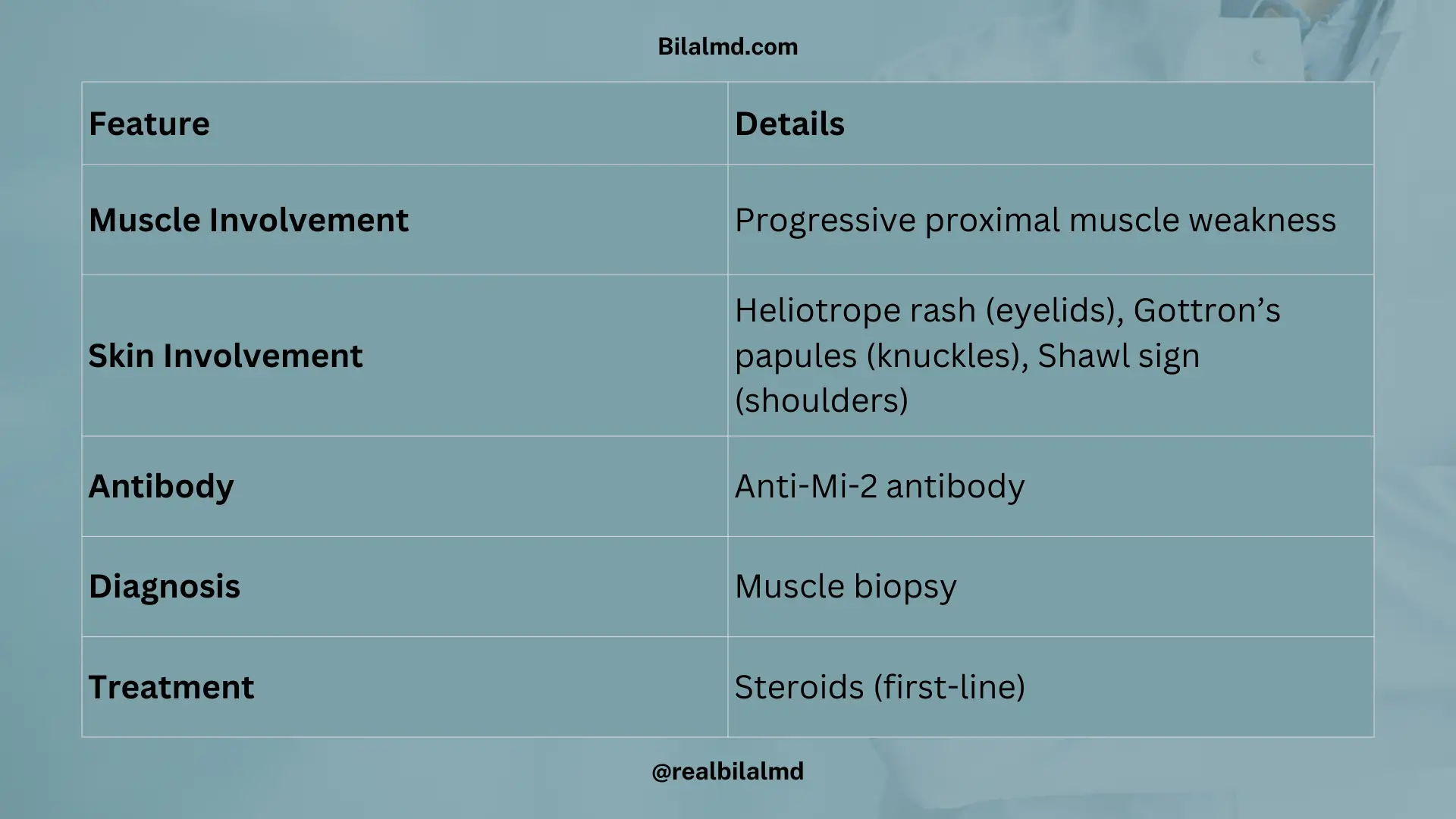
15. Dermatomyositis
Muscle involvement:
- Progressive muscle weakness (proximal > distal)
Skin involvement:
- Heliotrope rash → around eyelids
- Gottron’s papules → over knuckles
- Shawl sign → rash on shoulders
Antibody: Anti-Mi-2 antibody
Diagnosis: Muscle biopsy
Treatment: Steroids (first-line)
16. Systemic Lupus Erythematosus (SLE)
- Type: Autoimmune disease (multisystem involvement)
- Epidemiology:
- F > M
- Younger age group
Clinical Features
- Skin → Malar rash, photosensitivity
- Joints → Arthralgia
- Blood → Anemia
- Renal → Impairment (nephritis)
- Neuro → Neural involvement (seizures, psychosis)
- General → Fatigue
Laboratory
- ANA → Positive (sensitive)
- Anti-dsDNA → Positive (specific)
- Drug-induced SLE → Anti-histone antibody
Note
- Mild SLE (no renal, no neuro involvement) → Better prognosis
17. Systemic Sclerosis (Scleroderma)
- Pathology → Excess collagen (types I & III) → skin hardening
- Types:
- Limited (CREST syndrome) → Anti-centromere antibody
- C → Calcinosis
- R → Raynaud phenomenon
- E → Esophageal dysmotility
- S → Sclerodactyly
- T → Telangiectasia
- Diffuse → Widespread organ involvement
- Limited (CREST syndrome) → Anti-centromere antibody
- Tx → ACE inhibitors (esp. for renal crisis)
18. Sjogren Syndrome (autoimmune, exocrine destruction)
- Glands involved → Lacrimal & salivary → dry eyes + dry mouth
- Antibodies:
- Anti-Ro (SSA) → Positive
- Anti-La (SSB) → Decreased
- ANA → Positive
- Diagnostic test → Schirmer test < 5 mm
- Treatment:
- Artificial tears
- Pilocarpine (↑ secretions)
Check your NRE Step 1 result after completing the exam.