Beta cells: Located in the pancreas (in the islets of Langerhans) and involved in insulin production.
T cells: Part of the immune system, involved in adaptive immunity.
2. Infectious Mononucleosis:
Cause:
Epstein-Barr Virus (EBV).
Clinical Features:
Splenomegaly: Enlargement of the spleen due to infection.
T-cell Hyperplasia: An increase in T cells as part of the immune response to the viral infection.
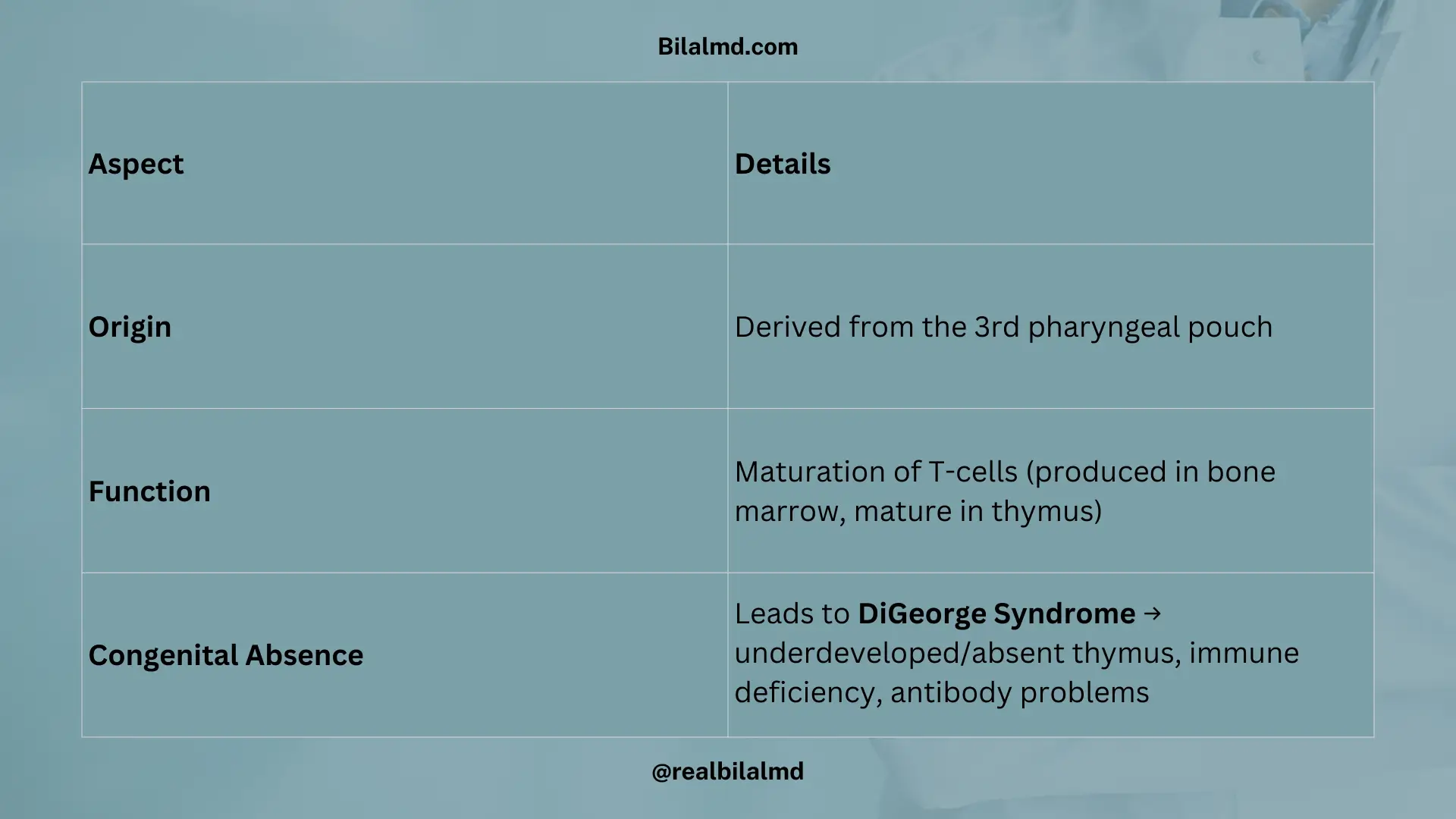
2. Thymus
Origin:
Derived from the 3rd pharyngeal pouch.
Function:
Responsible for the maturation of T-cells.
T-cells are made in the bone marrow, but they mature in the thymus.
Congenital Absence:
If the 3rd pharyngeal pouch is absent, it leads to DiGeorge Syndrome, a condition where the thymus is underdeveloped or absent, affecting immune function and causing antibody deficiencies.
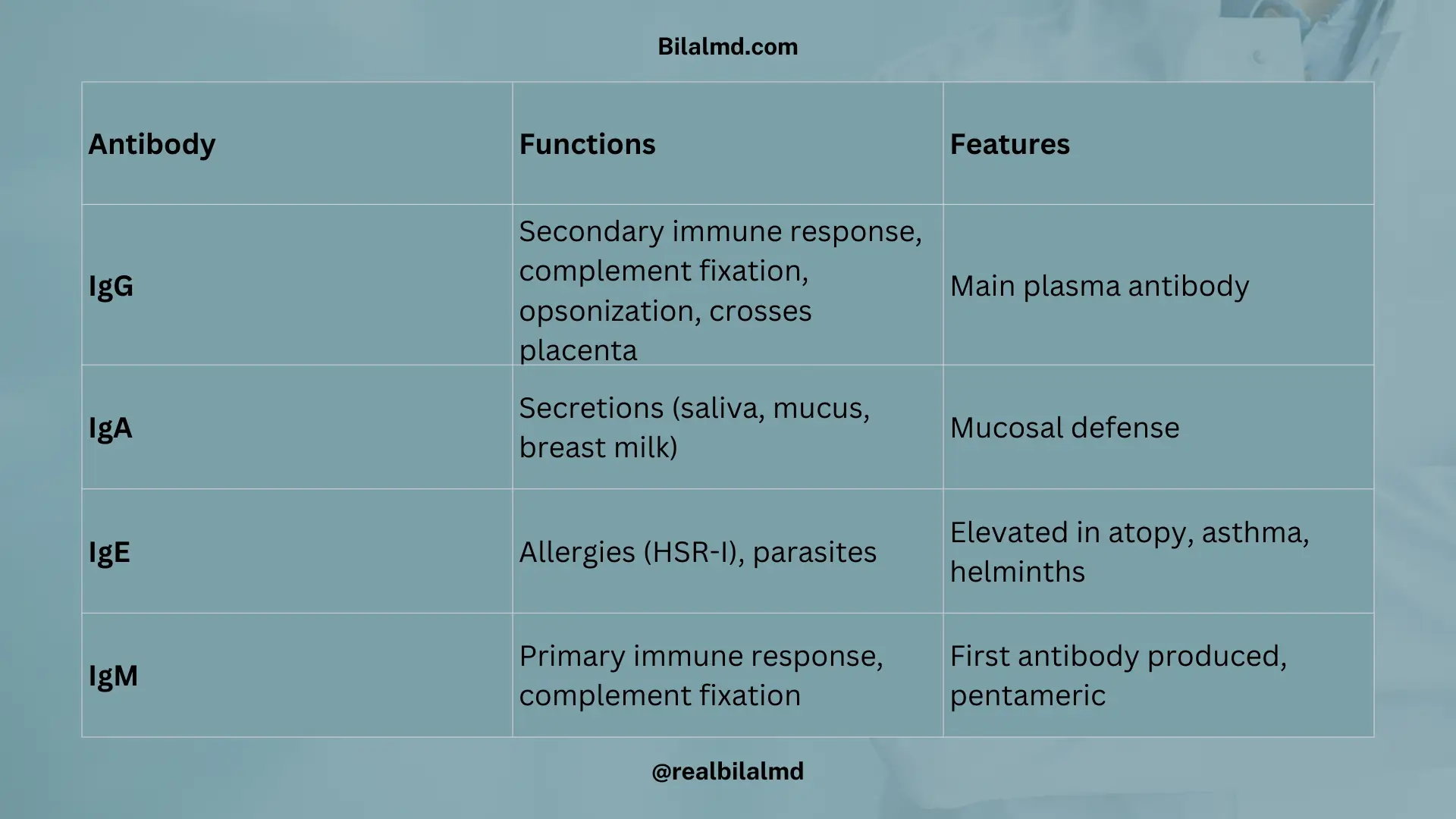
3. Antibodies and Immune Responses
Antibody
Function
Characteristics
IgG
– Secondary immune response – Crosses the placenta – Complement fixation – Opsonization – More in plasma
– Main antibody in secondary immune response – Helps fix complement and aids in opsonization – Crosses placenta to provide passive immunity
IgA
– Present in secretions (saliva, mucus, breast milk) – More produced but drains
– Found in mucosal membranes – Lower concentration in blood but crucial for mucosal immunity
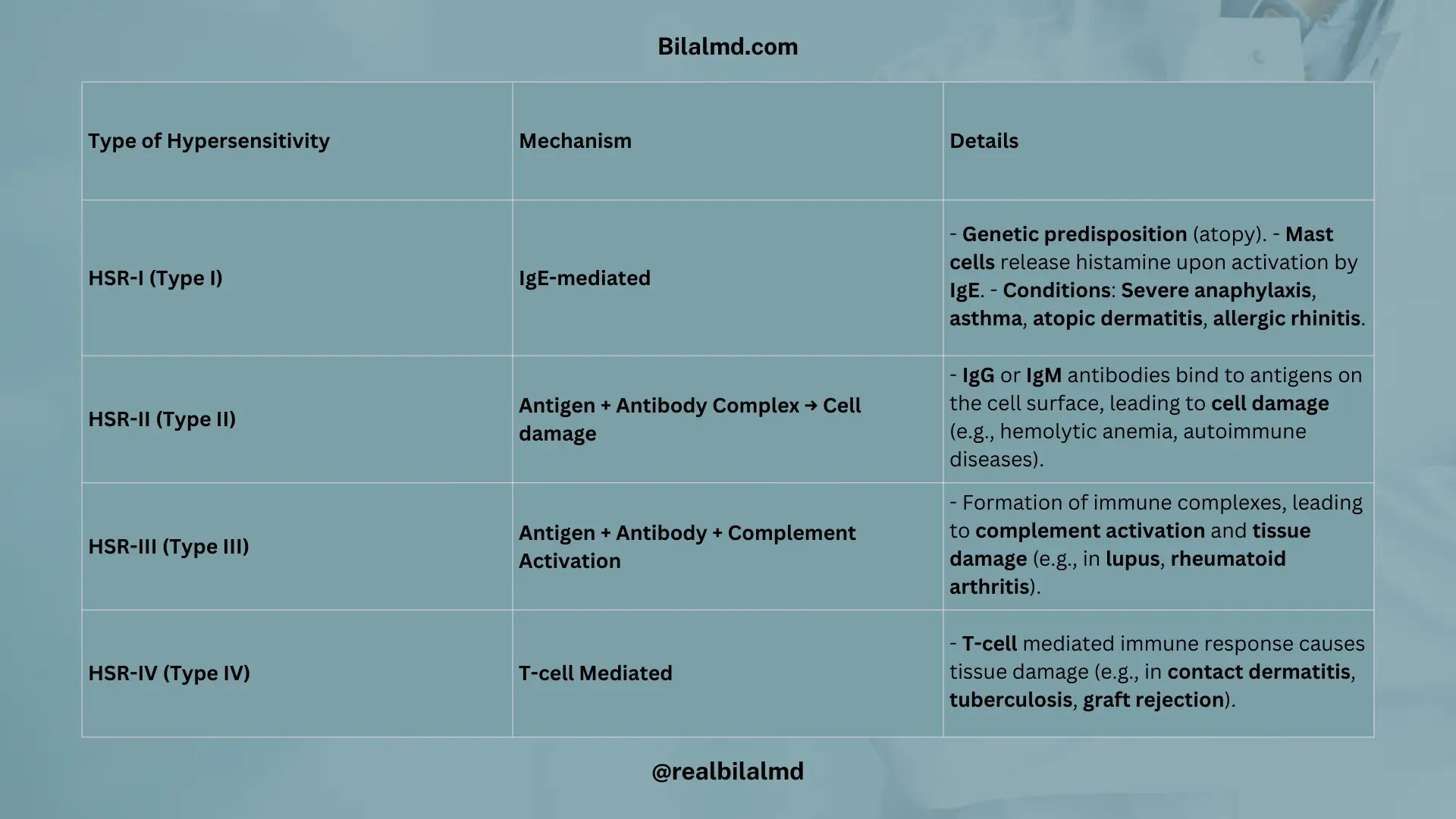
IgE
– Involved in HSR-1 (Type I hypersensitivity) – Plays a role in parasitic infections
– Involved in allergic reactions and parasite defense – Elevated in parasitic infections and allergies
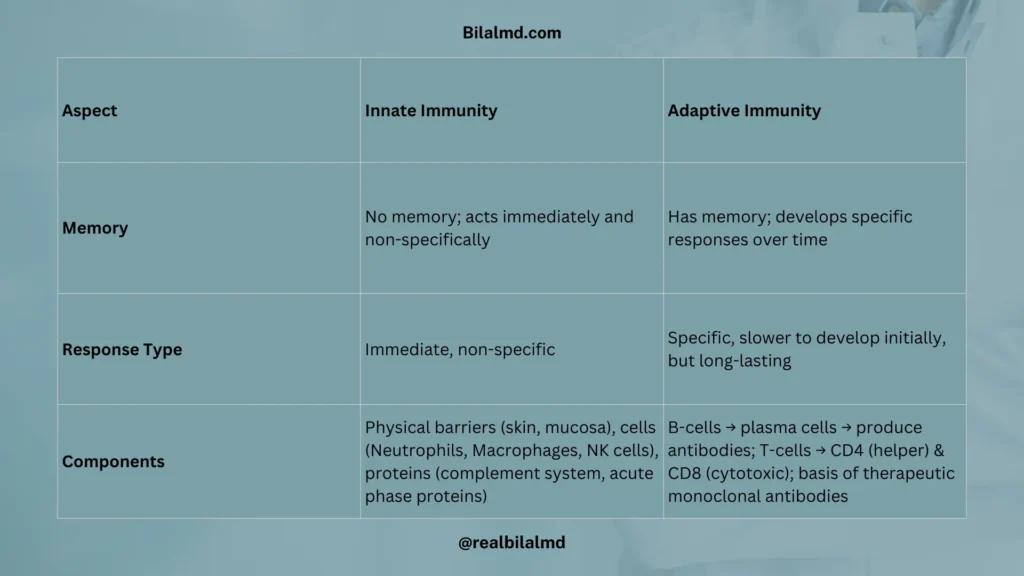
B-cells → mature into plasma cells → produce antibodies.
T-cells → CD4 (helper) and CD8 (cytotoxic).
Basis of therapeutic monoclonal antibodies.
1. Monoclonal Antibodies (Examples)
Drug
Target
Use
Denosumab
RANK-L
Osteoporosis
Omalizumab
IgE
Asthma (allergic)
Palivizumab
RSV F protein
RSV bronchiolitis prophylaxis
Eculizumab
C5 complement
Paroxysmal nocturnal hemoglobinuria (PNH)
Efalizumab
CD11a (LFA-1)
Psoriasis
Natalizumab
α4-integrin
Multiple sclerosis
Trastuzumab
HER2/neu receptor
HER2+ breast cancer, gastric cancer
Check your NRE Step 1 result after completing the exam.
Share
Manage Consent
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.