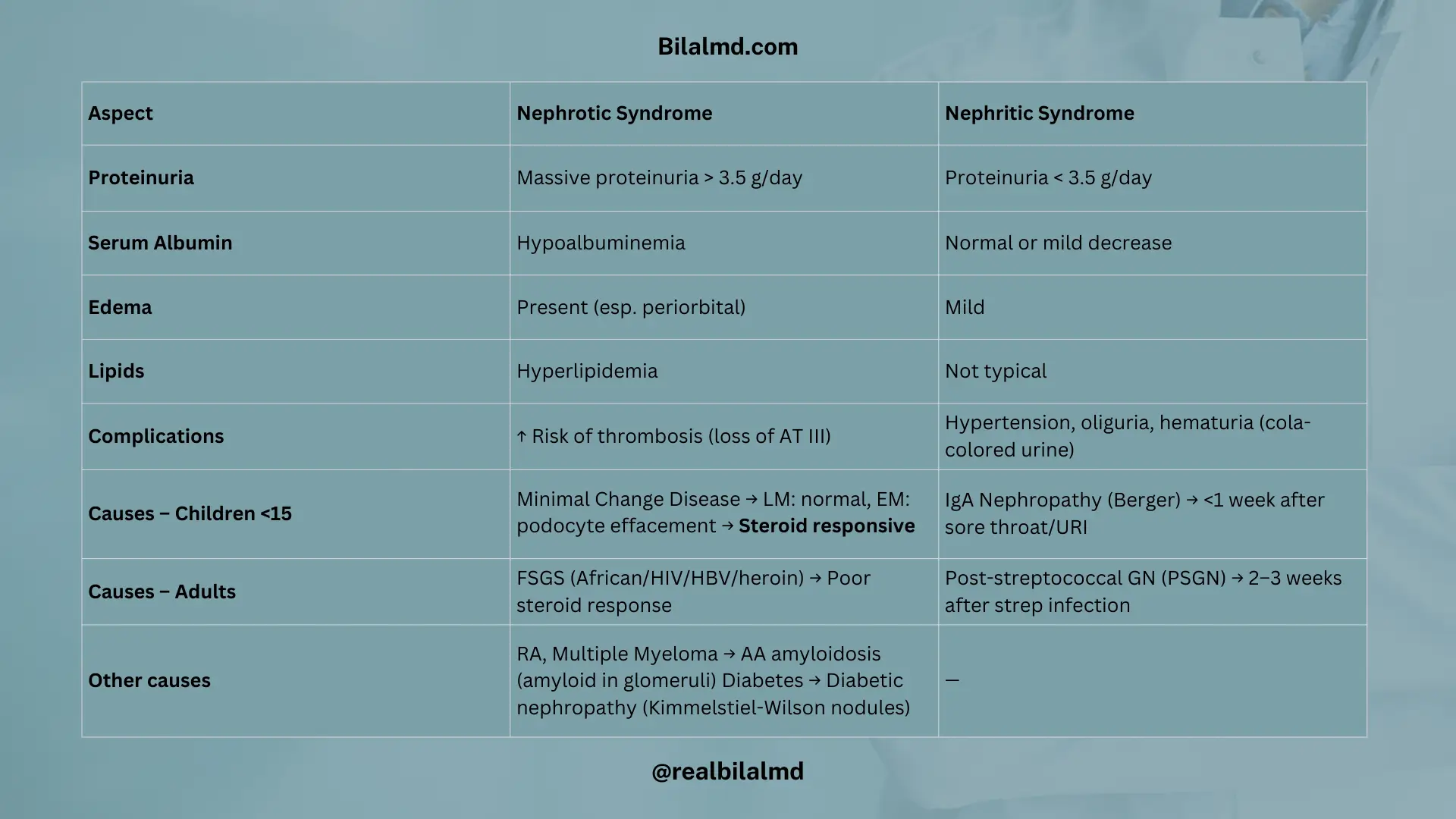
1. Nephrotic vs Nephritic Syndrome
Nephrotic Syndrome
- Massive proteinuria > 3.5 g/day
- Hypoalbuminemia
- Edema (esp. periorbital)
- Hyperlipidemia
- ↑ Risk of thrombosis (loss of AT III)
Causes:
- Children <15 yr → Minimal Change Disease → LM: normal, EM: effacement → Steroid responsive
- African/HIV/HBV/heroin → FSGS → Poor steroid response
- RA, Multiple Myeloma → AA amyloidosis → Amyloid in glomeruli
- Diabetes → Diabetic nephropathy → Kimmelstiel-Wilson nodules
Nephritic Syndrome (Inflammatory):
- Proteinuria < 3.5 g/day
- Hypertension
- Oliguria
- Hematuria (cola urine)
Post-infectious:
- <1 wk after sore throat/URI → IgA Nephropathy (Berger)
- 2–3 wks after strep → PSGN
2. Vasculitis
ANCA-associated:
- GPA (Wegener’s) → Kidney + Lung + Sinus, c-ANCA (PR3)
- Microscopic polyangiitis → Kidney + Lung (no sinus, no granuloma), p-ANCA (MPO)
- Churg-Strauss (EGPA) → Kidney + Asthma + Eosinophilia, p-ANCA
Anti-GBM:
- Goodpasture → Hematuria + Hemoptysis, Anti-GBM Ab → Tx: Plasma exchange
Hereditary nephritis:
- Alport (X-linked, Type IV collagen defect)
- Triad: No see (ocular), No pee (renal failure/hematuria), No hear (SNHL)
- Tx: ACEI/ARB
3. Acid–Base Balance & ABGs
- pH: 7.35–7.45
- pCO₂: 35–45 mmHg
- HCO₃⁻: 22–26 mEq/L
- pH ∝ HCO₃⁻ (metabolic), pH ∝ 1/CO₂ (respiratory)
- Anion gap = (Na⁺ + K⁺) – (Cl⁻ + HCO₃⁻) → Normal: 12–16
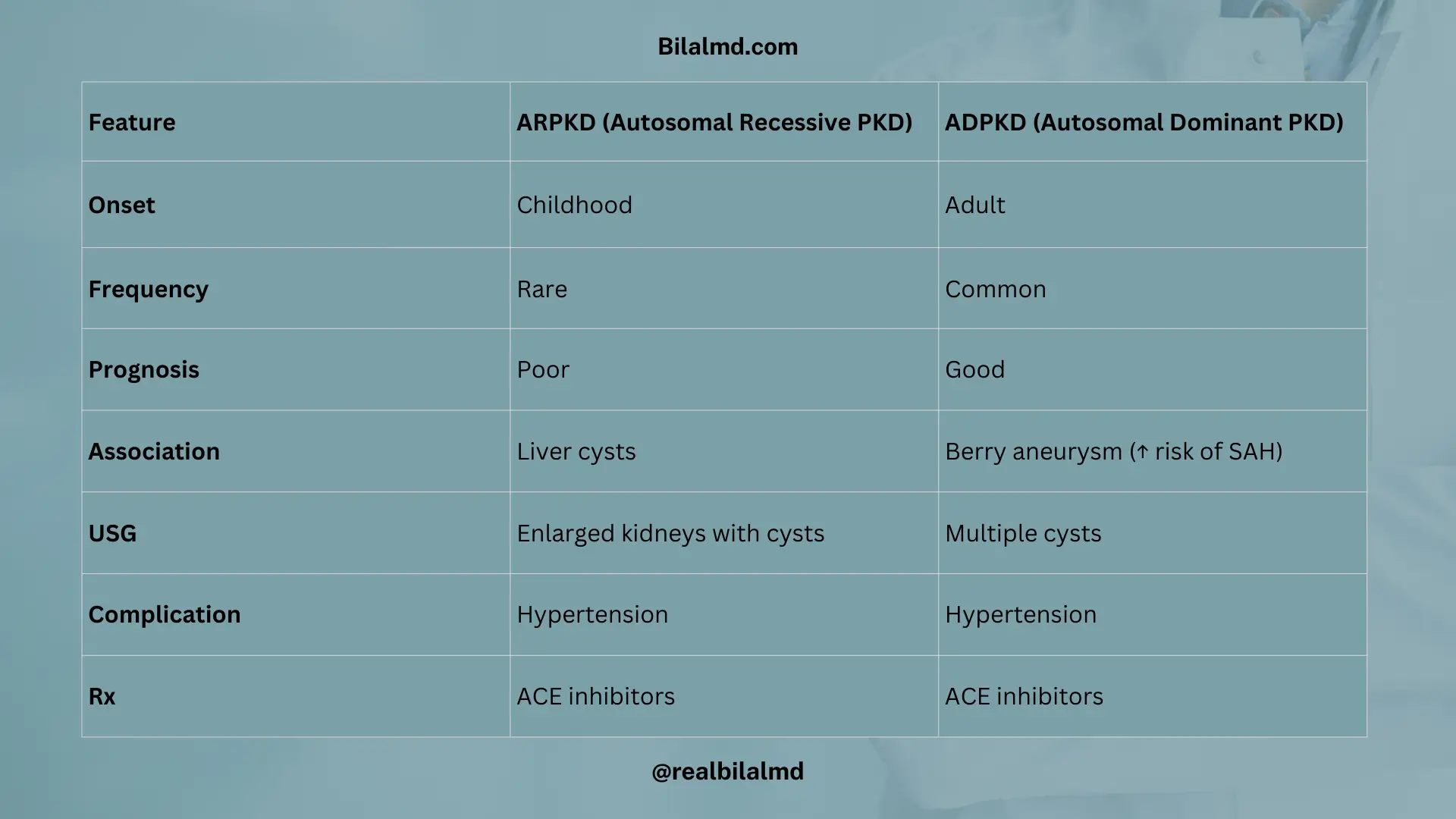
4. Polycystic Kidney Disease (PKD)
| Feature | ARPKD | ADPKD |
|---|---|---|
| Onset | Childhood | Adult |
| Frequency | Rare | Common |
| Prognosis | Poor | Good |
| Association | Liver cysts | Berry aneurysm (↑ SAH risk) |
| USG | Enlarged kidneys w/ cysts | Multiple cysts |
| Complication | HTN | HTN |
| Rx | ACE inhibitors | ACE inhibitors |
5. Hydronephrosis
- Dilatation of renal pelvis & calyces (obstruction/urine retention)
- Can cause tubular atrophy → RTA
RTA Types:
- Type 2 (proximal): ↓ HCO₃⁻ reabsorption, ↓ K⁺, ↓ Vit D → rickets/osteomalacia
- Type 1 (distal): ↓ H⁺ secretion, Urine pH >5.5, ↓ K⁺, ↑ Risk stones
- Type 4: Hypoaldosteronism, ↓ Na⁺, ↑ K⁺, ↓ BP, common in DM
Here are other materials for NLE NRE step 1
6. Acute Kidney Injury (AKI)
- Definition: ↓ GFR, ↑ Cr <3 months
| Type | Features | FENa |
|---|---|---|
| Prerenal | Hypoperfusion (shock, dehydration, HF) | <1% |
| Intrinsic | ATN, GN | >2% |
| Postrenal | Obstruction (stones, BPH) | >2% |

7. Chronic Kidney Disease (CKD)
- Definition: ↓ GFR or renal dysfunction >3 months
Features: HTN, Edema, Uremic pericarditis, Renal osteodystrophy (↓ Vit D → ↓ Ca), Normocytic anemia (↓ EPO)
Treatment:
- ACEI/ARB (slow progression, control BP)
- Calcitriol (Vit D)
- Diuretics (for overload)
- Avoid NSAIDs
- Erythropoietin (anemia)
- Dialysis (severe cases)
- Transplant (definitive)
8. Electrolyte Imbalances & ECG
- K⁺: 3.5–5.5
- ↑ → Tall T, wide QRS, prolonged PR
- ↓ → U waves
- Ca²⁺: 8–10
- ↑ → Short QT
- ↓ → Long QT
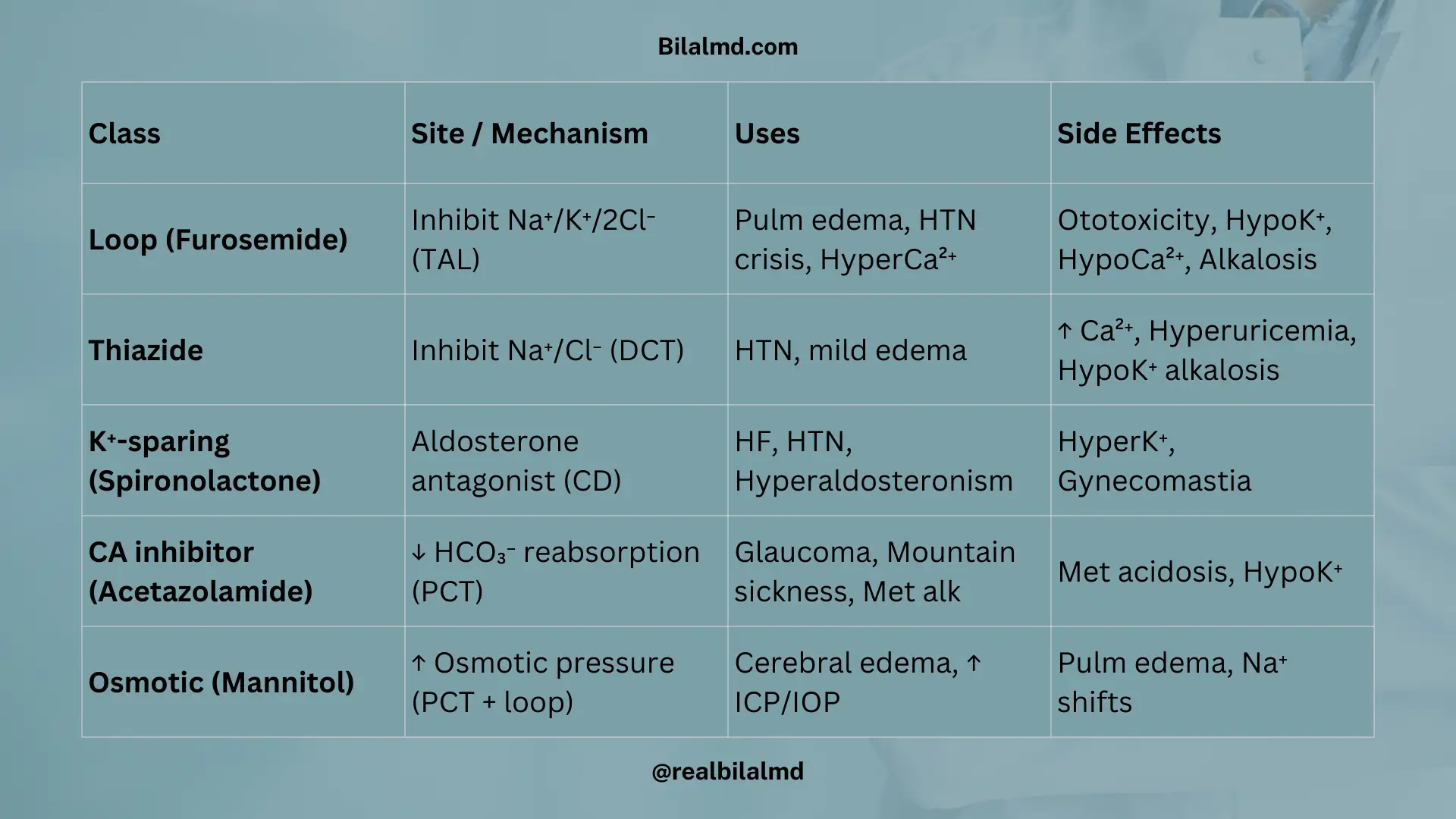
9. Diuretics
| Class | Site / Mechanism | Uses | Side Effects |
|---|---|---|---|
| Loop (Furosemide) | Inhibit Na⁺/K⁺/2Cl⁻ (TAL) | Pulm edema, HTN crisis, HyperCa²⁺ | Ototoxicity, HypoK⁺, HypoCa²⁺, Alkalosis |
| Thiazide | Inhibit Na⁺/Cl⁻ (DCT) | HTN, mild edema | ↑ Ca²⁺, Hyperuricemia, HypoK⁺ alkalosis |
| K⁺-sparing (Spironolactone) | Aldosterone antagonist (CD) | HF, HTN, Hyperaldosteronism | HyperK⁺, Gynecomastia |
| CA inhibitor (Acetazolamide) | ↓ HCO₃⁻ reabsorption (PCT) | Glaucoma, Mountain sickness, Met alk | Met acidosis, HypoK⁺ |
| Osmotic (Mannitol) | ↑ Osmotic pressure (PCT + loop) | Cerebral edema, ↑ ICP/IOP | Pulm edema, Na⁺ shifts |