Learn the history of present illness in clinical medicine. Step-by-step HPI format, symptom-based questions, and patient history template.
History taking is a structured conversation between the doctor and the patient to understand what is making the patient unwell. It is the foundation of clinical history taking and forms the first step before physical examination or investigations.
To collect accurate information, the doctor must adapt their language and tone according to the patient’s age, background, and education level.
Simple Guidelines for History Taking
The goal of medical history taking is not just to gather facts but to build trust and communication. A good clinician listens carefully, shows empathy, and guides the conversation naturally.
General Approach
- Be kind, calm, and respectful. Maintain a friendly and confident tone.
- Always introduce yourself and explain your role.
- Speak in the patient’s language. Use simple words; avoid technical or medical terms.
- Be polite, don’t interrupt personal activities (for example, if the patient is eating, wait or return later).
Listening Before Asking
Let the patient tell their story freely before you ask focused questions. This is the most important part of the history of present illness (HPI) understand
- how the illness started
- how it progressed
- what makes it better or worse.
Order matters: Listen first → Ask next → Write last.

If you need to interrupt, do so gently and only when necessary.
Ask Open Questions, Not Leading Ones
- ❌ Bad: “Do you have chest pain?” (yes/no)
- ✅ Better: “Where do you feel the pain?”
Use open-ended patient history taking questions to encourage detailed responses. Get clear, specific descriptions such as “burning pain before or after meals” instead of vague words like “acidity.”
Writing During History Taking!
Avoid writing constantly while the patient speaks; it can make them feel ignored. Maintain eye contact and attention.
If needed, write down short notes quietly, then write the full record immediately after the interview before starting the physical examination.

This ensures you remember the key details of the history of present illness and other sections.
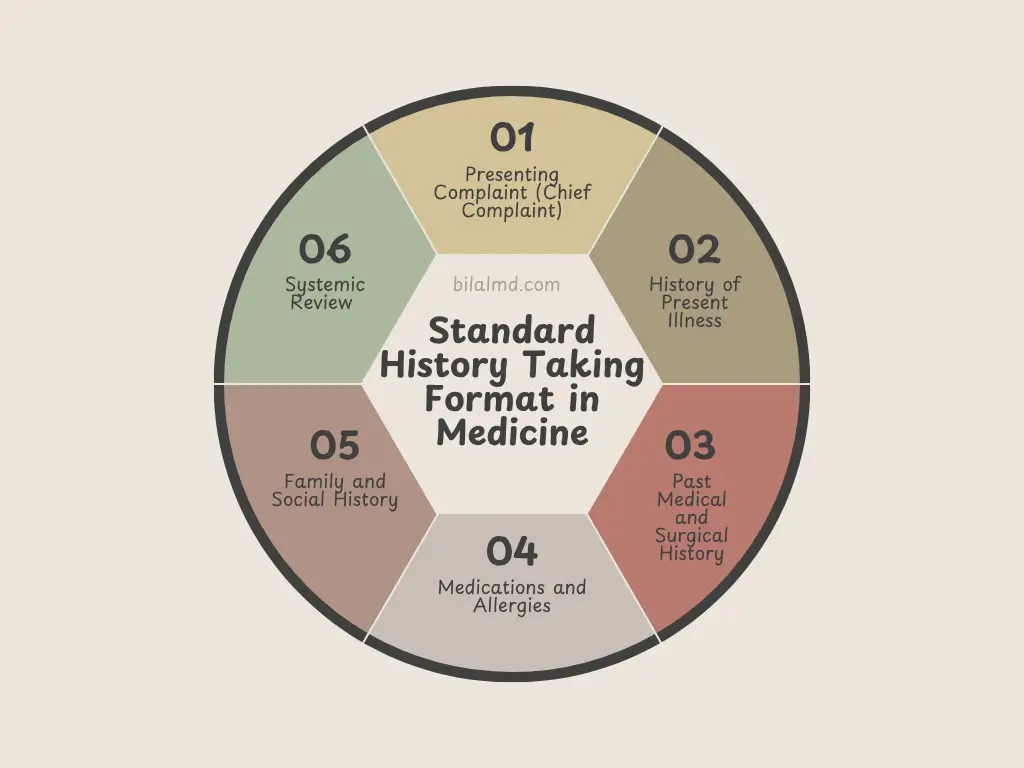
Standard History Taking Format in Medicine
Even though patients rarely talk in a structured way, doctors should record the data in a consistent format:
- Presenting Complaint (Chief Complaint)
- History of Present Illness (HPI)
- Past Medical and Surgical History
- Medications and Allergies
- Family and Social History
- Systemic Review (Review of Systems)
This format is the backbone of clinical medicine methods and should be followed for every case.
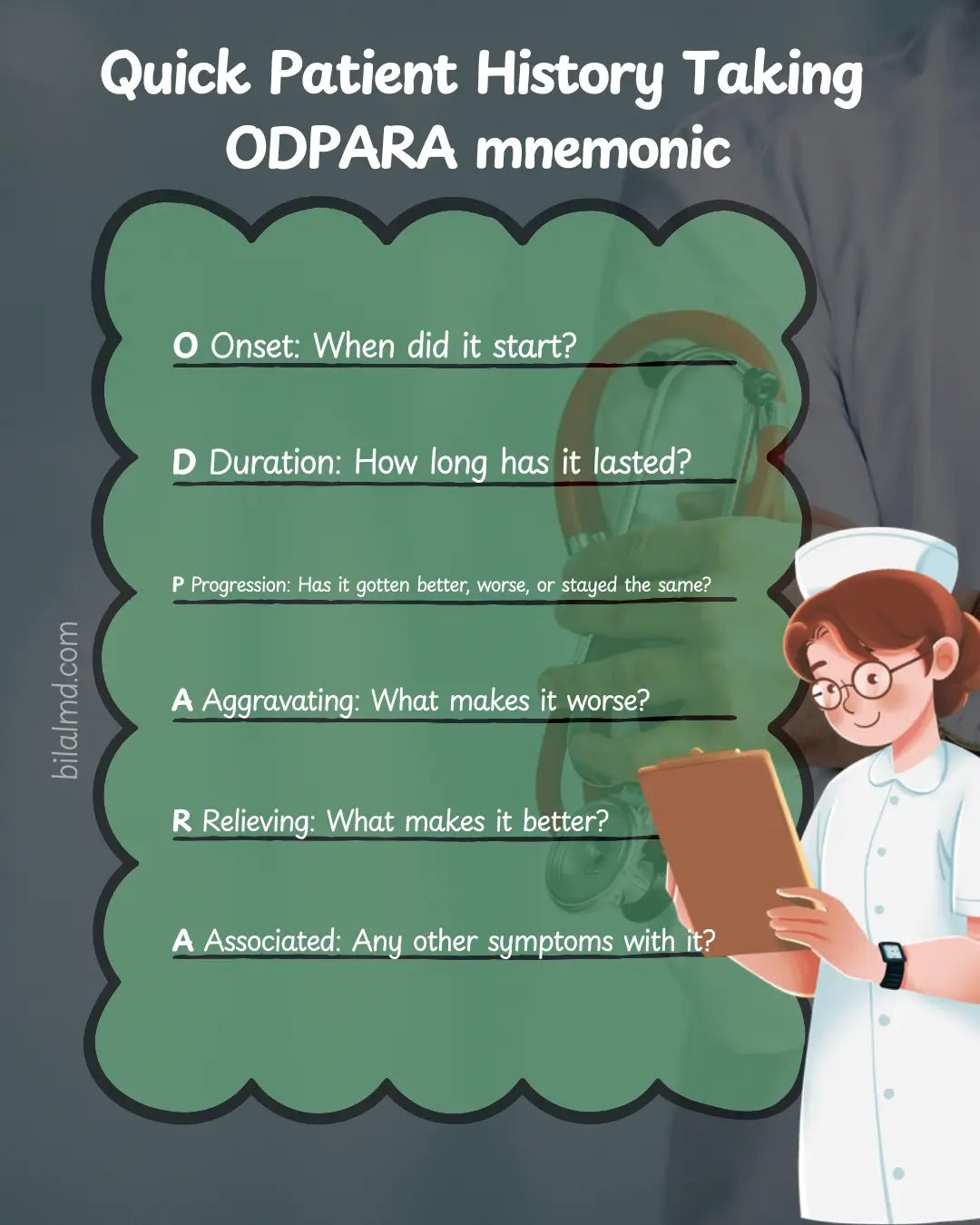
Quick Patient History Taking Questions You Can Use
Here is a mnemonic that fit almost every clinical scenario:
ODPARA
| Component | Meaning | Example Question |
|---|---|---|
| O – Onset | When did it start? | “When did you first notice this problem?” |
| D – Duration | How long has it lasted? | “Has it been continuous or off and on?” |
| P – Progression | Has it gotten better, worse, or stayed the same? | “Has it changed since it started?” |
| A – Aggravating factors | What makes it worse? | “Does anything trigger or worsen the symptoms?” |
| R – Relieving factors | What makes it better? | “Have you tried anything that eases it?” |
| A – Associated symptoms | Any other symptoms with it? | “Do you have fever, nausea, or anything else with this?” |
These questions for history of present illness encourage open communication and give you a complete picture of the patient’s condition.
Complete History Taking Format in Medicine
Medical history taking is the first and most essential step in clinical diagnosis. A well-structured format helps doctors collect accurate information, understand the history of present illness (HPI), and identify risk factors and patterns related to disease.
Remember: HIPS-TO-FORM – it contains the complete format for taking history across all systems.
| Letter | Section |
|---|---|
| H | History of Present Illness |
| I | Identification |
| P | Presenting Complaints |
| S | Systemic Inquiry |
| T | Treatment History |
| O | Occupational History |
| F | Family History |
| O | Personal & Social History |
| R | Reproductive / Menstrual History |
| M | Medical & Past History |
Below is a standard clinical history taking format used in most hospitals and medical schools.
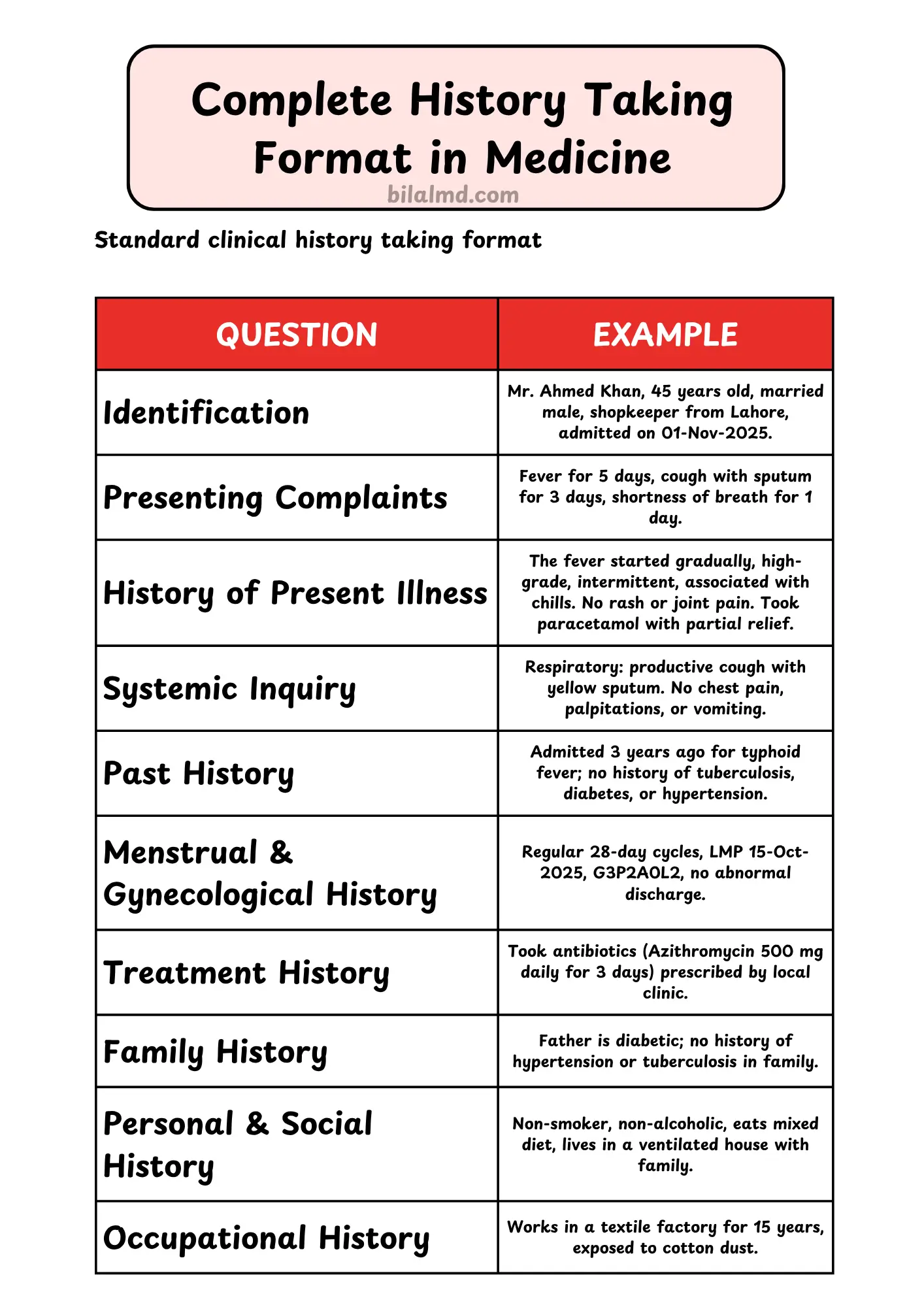
1) Identification
- Name, age, sex, marital status, occupation, address. Add father’s/husband’s name if needed to distinguish people.
- If age is uncertain, estimate (appearance, age at marriage, eldest child’s age).
- Why it matters:
- age/sex/region/job often point to likely diseases. Like SLE is common in female and sarcoidosis is common in factory workers.
2. Presenting Complaints (PC)
Record the chief complaints that brought the patient to the hospital at present time. Write them in the sequence of onset and duration.
- Example: “Burning epigastric pain – 10 days; Vomiting – 2 days.”
- If a symptom is recurrent, state so: “Recurrent left flank pain – 6 months.”
This section summarizes what the patient feels is wrong, which leads into the detailed history of present illness.
3. History of Present Illness (HPI)
This is the most crucial part of the record. Use the patient’s own words to describe each symptom in detail this is your history of present illness template. Use ODPARA mnemonic like we did before;
- Onset – When it started
- Character & Site – Type, location, radiation of pain
- Severity & Impact – How it affects daily life
- Timing/Progression – Continuous or intermittent
- Triggers/Relievers – What worsens or improves it
- Associated Symptoms – Fever, nausea, breathlessness, etc.
If multiple symptoms occur, describe the latest episode first, then give an overview of the pattern since onset.
Avoid writing premature diagnoses. Write “shortness of breath at night” not “PND” unless clinically confirmed. For students, practice using this HPI format example to build structured, logical notes.
4) Systemic Inquiry
The patients will tell only those symptoms that they think are important and need attention. They either think other symptoms are non-important or they forget. To make sure they don’t forget, ask questions about all the systems. Don’t repeat questions that have already been asked. Start from the head to toe.
Use the GGENCURMS mnemonic.
- General: appetite, weight change, sleep, energy.
- GI: nausea, vomiting, abdominal pain, heartburn, swallowing trouble, diarrhea/constipation, black/tarry stools, jaundice.
- Endocrine: Increase of urine/thirst/hunger, heat/cold intolerance, weight change, sweating, palpitations.
- Neuro: weakness, numbness/tingling, headaches, dizziness, blackout/fits, vision changes/double vision, vomiting.
- Cardio: breathlessness, palpitations, chest pain, ankle swelling.
- Urinary: flank pain, burning, blood in urine, frequency, too much/too little urine, night urination, gravel/stones.
- Respiratory: cough, sputum, blood in sputum, wheeze, chest pain.
- Musculoskeletal: joint pain/stiffness/swelling, limited movement.
- Skin: rashes, itching, color changes.

If the patient can’t give history (child, confusion, unconscious, seizures), get it from a reliable witness.
5) Past History
Be Cool, Make Chronic Records – Always thoroughly review a patient’s past. Remember mnemonic B-C-M-C-R.
| Letter | Category | Key Details |
|---|---|---|
| B | Birth history | Spontaneous / assisted / cesarean; home or hospital |
| C | Congenital anomalies | Any birth defects, developmental issues |
| M | Major illnesses / surgeries / hospitalizations / accidents | With approximate dates |
| C | Chronic diseases | Hypertension, diabetes, TB, asthma, arthritis, etc. |
| R | Residence or travel abroad | For infections or exposure risk |
Knowing past diseases helps identify comorbidities that may influence the present illness.
6. Menstrual & Gynecological History (when relevant)
Ask A DRESS M – every woman wears her own menstrual DRESS!
| Letter | Category | Details |
|---|---|---|
| A | Age at menarche | When periods first started |
| D | Duration | How many days bleeding lasts |
| R | Regularity | Regular or irregular cycles |
| E | Endometriosis-like pain | Pain during menstruation – site & timing |
| S | Spotting / Intermenstrual bleeding | Bleeding between periods or after intercourse |
| S | Senescence (Menopause) | Age at menopause & post-menopausal bleeding |
| M | Menstrual cycle length | Interval between periods |
7) Treatment History
Many patients forget exact drug names they may recall only size, color, or shape. Ask to see prescriptions, packaging, or leftover medicines.
- Drug name, dosage, duration
- Response to treatment
- Side effects or allergies (e.g., penicillin, captopril)
- Non-compliance (not completing medication) is common. Always find out why affordability, side effects, or misunderstanding.
Drug history also provides diagnostic clues and identifies possible drug-induced symptoms.
8) Family History
Ask about:
- Health of Parents, siblings, and children
- Similar illnesses or chronic conditions of family(HTN, DM, IHD, asthma, TB, arthritis)
- Cause of death in deceased relatives
- If genetic disease suspected, ask about uncles, aunts, or cousins.
9) Personal & Social History
This section reveals lifestyle and emotional factors affecting health.
Ask about:
- Economic status – affordability of tests and treatment
- Family relationships – stress and support levels – Stress from family conflict can elevate cortisol, causing gastrointestinal issues.
- Addictions – smoking, alcohol, recreational drugs
- Sleep disturbance or anxiety
- Current and previous occupation
10) Occupational History
Ask about:
- Exposure to chemicals, dust, or radiation
- Duration of work and safety measures used
- Protective equipment or lack thereof
Certain diseases are linked to specific occupations, such as pneumoconiosis in miners and asbestosis in construction workers.
Common QUESTIONS ABOUT CARDINAL SYMPTOMS
1) Pain, what to ask (move from open → focused)
For pain assessment the standard and most widely accepted mnemonic is: SOCRATES

| Letter | Meaning | What to Ask |
|---|---|---|
| S | Site | “Where exactly is the pain?” |
| O | Onset | “When did it start? Was it sudden or gradual?” |
| C | Character | “What does it feel like sharp, dull, burning, stabbing?” |
| R | Radiation | “Does the pain move anywhere?” |
| A | Associated symptoms | “Do you have nausea, fever, sweating, etc.?” |
| T | Time / duration | “How long have you had it? Is it constant or intermittent?” |
| E | Exacerbating / relieving factors | “What makes it better or worse?” |
| S | Severity | “On a scale of 1–10, how bad is it?” |
A) Site of pain (exact location)
- “Point with one finger where exactly is the pain?”
- Typical sites:
- Duodenal ulcer felt at epigastrium
- Ischemic heart disease felt across retrosternal (across the sternum, not just precordium)
- Reflux esophagitis is burning along the sternum
- Across sternal = deep, broad pressure (heart).
- Along sternal = surface, burning track (acid reflux).
B) Intensity (severity)
Intensity of pain varies in different people
Ask;
- “How bad on a 0–10 scale?
- Does it wake you from sleep or make you restless?”
- Very severe pain often with pancreatitis, MI, or colicky pain.
C) Radiation (does it travel?)
The pain moves from one area to another.
- Cholecystitis: pain in right hypochondrium → right costal margin → back
- Cardiac ischemia: pain to chest → to left arm to jaw or neck
D) Migration / Shift of pain
- “Did it start somewhere else and move?”
- Appendicitis: periumbilical pain → right iliac fossa (umbilical pain fades as RIF pain appears)
E) Referred pain
- Pain felt at other area than the main site due to same nerve supply.
- Cholecystitis: right shoulder (phrenic/diaphragmatic referral)
F) Duration of each episode
Some pains is felt for a specific time period.
- Angina: usually < 30 minutes
- MI pain: typically > 30 minutes and persistent
G) Character (quality)
- People use different terms to describe same pain.
- Heaviness/pressure, burning, dull/aching, throbbing, stabbing/cutting, gripping/cramping, pricking, colicky
Colicky
- Colic = wave-like pain from a hollow organ trying to push past an obstruction. (pain-free intervals e.g., gas, feces)
- Intestinal colic: sharp waves with pain-free intervals (no pain between contractions – Ureteric colic).
- Ureteric colic: pain eases between spasms but doesn’t fully disappear (stone irritation continues).
H) Frequency / periodicity
Ask;
- “Do pain attacks come and go? Are pain-free gaps getting shorter/longer?”
- Duodenal ulcer: weeks of pain → symptom-free period → recurrence.
I) Special time of occurrence
some pain has their special characters like in
- Scabies: itching before sleep
- Duodenal ulcer: wakes patient after midnight, rarely present on rising
- Sinusitis: worst a few hours after getting up
- Migraine: commonly around menses
J) Aggravating factors
Anything that increases the pain.
- Movement → joint/muscle pain
- Angina: exertion, cold, stress
- Peptic ulcer: tea/spices
- Pleuritic pain: deep breath/cough
K) Relieving factors
Some pain has their relieving facors like
- Angina relieved by rest, sublingual nitrates
- Duodenal ulcer relieved by food or antacids
L) Associated features
There is 1 main illness and other are supporting factors for the main illness like;
- Cholecystitis is associated with abdominal pain + vomiting
- MI is associated with chest pain + palpitations + sweating
2) Fever – how to structure the questions
Definition: > 98.4°F (37°C). Normal variation: lower morning, higher evening. If there is any issue fever is common. if someone come with fever ask them following question.
A) Mode of onset
- Sudden (acute infections): malaria, pneumonia, UTI → “I was fine yesterday; high fever today.”
- Insidious (chronic infection/malignancy): slow, low-grade, prolonged → “Low fever for weeks, getting worse.”
B) Rigors or chills
Rigors and chill indicate a sudden rise in body temperature. Ask;
- “Do you get shaking chills?”
- Points to rapid temp rise (malaria, pyelonephritis, severe pneumonia, sepsis).
C) Grade (how high)
- High-grade: acute bacterial illness more likely
- Low-grade: chronic infection, inflammatory disease, malignancy
Pattern of fever
There are 4 patterns of fever.
Mini-mnemonic (Cool Riders In Race): C R I R
- Continuous
- Remittten
- Intermitten
- Relapse
D) Pattern of fever (ask them to keep a simple chart if unclear)

Continuous Fever
- Temp remains above normal all day; does not touch baseline.
- Classic: Typhoid (gradual rise → sustained 102–104°F).
- Even at night or in the morning, it remains elevated.
Remittent Fever
- Always above normal but fluctuates > 2°C (~3°F) in 24 h. (101°F in the morning → 104°F in the evening)
- Many infections fit here; patient feels a bit better when it dips, but it never normalizes.
- Fever is still there but never completely normal.
Intermittent Fever
- Fever spikes for hours then returns to normal (afebrile interval).
- Malaria: chills → fever → sweats → normal period.
- TB: often evening rise (low-grade, night sweats).
- Subtypes: Quotidian (fever daily), Tertian (fever every other day), Quartan (fever every third day).
Relapsing Fever
- Days of fever → several fever-free days → fever returns; cycles often similar length (e.g., 5 on / 5 off).
- Seen with some infections and hematologic conditions.
E) Associated symptoms
- Ask other symptoms to guide differentials like:
Lymph nodes (often painless), rash, sore throat, cough, dysuria, headache, weight loss, night sweats.
Common Questions About Weight Loss, Mass, and Edema
1. Weight Loss
When a patient reports losing weight, always start by determining how much and over what period.
Step 1: Confirm the Weight Loss
- If a previous weight is known → weigh the patient again and calculate the difference.
- If no record exists → ask how much the patient feels they have lost and since when.
- Example: “I used to weigh 70 kg and now I’m 62 kg over 3 months.”
Step 2: Ask About Appetite
Because weight loss + appetite together often point toward the underlying disease.
Two key patterns:
- Weight loss with normal or increased appetite → points toward metabolic or endocrine disorders:
- Diabetes Mellitus (DM)
- Thyrotoxicosis (Hyperthyroidism)
- May also occur in malabsorption syndromes (weight loss + chronic diarrhea)
- Pro tip: In history taking, always ask about appetite, bowel habits, and fatigue together, these help distinguish endocrine from infectious causes.
- Weight loss with decreased appetite → suggests chronic infections such as:
- Tuberculosis (TB)
- HIV
- Malignancy
- Associated symptoms: fever, night sweats, chronic cough
2. Mass (Swelling or Lump)
A mass or lump can appear anywhere in the body. To remember what to ask, use the mnemonic SAD FPP:
S – Site (Where exactly is the lump located?)
A – Age / Appearance (When did it first appear? How does it look or feel?)
D – Duration / Growth (How long has it been there? Has it recently increased in size?)
F – Fever (Any fever or signs of infection around the lump?)
P – Pain (Is it painful or tender to touch?)
P – Pressure symptoms (Any trouble swallowing, breathing, or moving due to pressure from the mass?)
3. Edema (Swelling)
Edema means abnormal fluid accumulation, either generalized or localized. Identifying the site and sequence of swelling is crucial during clinical history taking.
Step 1: Site and Extent
- Generalized edema: whole body swollen common in nephrotic syndrome or severe malnutrition
- Localized edema: only one region affected typical of heart failure (CCF) or venous obstruction
Step 2: Sequence “Where did it start?”
- Around the eyes (periorbital swelling): often due to renal disease
- Feet or legs first: suggests congestive cardiac failure (CCF)
Step 3: Ask for Associated Symptoms
- Breathlessness → heart failure (CCF)
- Loss of appetite, vomiting, less urine → kidney failure
- Indigestion, diarrhea → malabsorption
- Abdominal swelling (distension) → liver disease (cirrhosis)
Remember: not all swelling means fluid overload — always relate edema to the underlying history of present illness (HPI).
1. Dyspnea (Breathlessness)
Two main types:
- Exertional Dyspnea – shortness of breath during activity (walking, stairs, running)
- Dyspnea at Rest – breathlessness even without activity; may occur suddenly (e.g., asthma attack)
When asking about Exertional Dyspnea:
- Duration: “How long have you been short of breath?”
- Severity: “What activity brings it on walking, climbing, or light work?”
- Progression: “Is it getting worse? Do you get breathless with less effort now?”
- Night attacks: Sudden breathlessness at night → Paroxysmal Nocturnal Dyspnea (PND)
- Lying flat: Worse on lying down → Orthopnea
- Associated symptoms:
- Cough/sputum → lung disease
- Palpitations/chest pain → cardiac disease
- Sweating/anxiety → stress or heart failure
Important background questions:
- History of chest pain → ischemic heart disease
- Hypertension → possible heart failure
- Fever with joint pain (past) → rheumatic fever → valvular heart disease
Dyspnea at Rest (Asthma or Bronchospasm):
Ask:
- Age of onset
- Wheezing (whistling sound)
- Attack frequency and severity
- Change in pattern since onset
- Allergies: skin rash or nasal allergy
- Family history of asthma/allergy
- Regular medication needed for symptom-free days
2. Palpitations (Awareness of Heartbeat)
- When: At rest or during activity?
- Duration: How long does each attack last?
- Pattern: Starts/stops suddenly or gradually?
- Associated symptoms:
- Breathlessness
- Chest pain
- Sweating
- Weight loss or heat intolerance → Thyrotoxicosis
3. Cough
- Duration: “How long have you been coughing?”
- Timing: Day or night?
- Type: Dry or productive?
- Sputum: color, amount, smell, worse in the morning?
- Blood: Is it mixed with sputum or pure? How much, how often?
- Cough with blood (hemoptysis) may indicate tuberculosis, bronchiectasis, or malignancy.
4. Vomiting
- Duration & frequency
- Relation to meals: before or after eating?
- Timing: morning or night?
- Weight loss: long-standing vomiting leads to malnutrition
- Character: color, smell, contents
- Blood (hematemesis): fresh red or dark brown?
- Black stools (melena): suggests upper GI bleed
- Other symptoms: pain, distension, constipation
- If the vomit contains food eaten 2–3 days ago → think achalasia cardia.
5. Diarrhea
- Duration: acute or chronic
- Frequency: how many stools per day
- Quantity: bulky or small, difficult to flush (→ malabsorption)
- Consistency: watery, loose, or rice-water (→ cholera)
- Blood/mucus present?
- Tenesmus: feeling of incomplete evacuation
- Relation to food: others ill from same meal? (→ food poisoning)
- At night: nocturnal diarrhea → organic disease (e.g., ulcerative colitis)
- Associated: fever, pain, vomiting, weight loss
6. Constipation
- Usual habit: “How many times per week?”
- Duration: new or chronic
- Change in pattern: recent change is important
- Blood in stool?
- Alternating diarrhea and constipation? (→ IBS)
- Drugs or diet change?
- Other symptoms: abdominal pain, distension, vomiting, weight loss
7. Dysphagia (Difficulty Swallowing)
- Duration
- Solids or liquids: which is harder?
- Progressive: getting worse?
- Sensation: “Does food get stuck somewhere?” where exactly?
- Painful swallowing?
- Weight loss?
- Vomiting of old food (2–3 days) → Achalasia cardia
- Heartburn or acidity → GERD or reflux esophagitis
8. Jaundice
Ask about:
- Pain right upper abdomen:
- Mild, continuous → hepatitis
- Severe, colicky → gallstones
- Loss of appetite
- Smoker losing taste for cigarettes → hepatitis
- Color changes: dark urine, pale stool
- Itching → cholestasis (bile blockage)
- Weight loss → malignancy
- History of: injections, blood transfusions → Hepatitis B/C
- Contact with jaundiced person → Hepatitis A/E
- Family history → inherited jaundice disorders
9. Polyuria (Passing Excessive Urine)
Differentiate from frequency:
- Polyuria: large volume each time
- Frequency: small volumes, many times
Ask about:
- Duration
- Thirst (polydipsia)
- Appetite: increased/decreased/normal
- Diuretic use?
- Night urination (nocturia)?
Polyuria + polydipsia + increased appetite = Diabetes Mellitus
10. Hematuria (Blood in Urine)
- Duration of blood
- Color of urine: red, brown, or smoky
- Timing of blood: start/middle/end of urination
- Associated: fever, burning, lower abdominal or flank pain
- Painful hematuria → infection; Painless → malignancy until proven otherwise.
11. Seizures (Fits)
Ask both patient and eyewitness if possible:
- Age at first attack
- Aura: any warning before fit
- Consciousness: lost or not
- Movements: stiff (tonic) or jerky (clonic)
- Localized or generalized?
- Tongue bite / incontinence?
- Fall or injury?
- Duration of fit
- After effects: sleep, headache, weakness
- During sleep or daytime?
- Interval between attacks?
- Associated: fever, vomiting, ear infection, head trauma, birth injury
12. Weakness or Paralysis
- Area involved: one limb (monoplegia), one side (hemiplegia), both legs (paraplegia)
- Degree: complete or partial
- Onset: sudden (stroke) or gradual (neuropathy)
- Progression: static or worsening
- Other symptoms: headache, vomiting, fits, speech or vision issues, numbness
- Risk factors: hypertension, diabetes, smoking, heart disease
- Previous episodes: and recovery outcome
- Family history: stroke or vascular disease
13. Headache
- Site:
- Top (vertex) → psychogenic
- Frontal/occipital → organic
- Severity & duration
- Continuous or episodic?
- Timing:
- Night: cluster headache
- Morning (few hours after waking): sinusitis
- Triggers: stress, menstruation, foods (cheese, caffeine), posture (bending forward)
- Relief: analgesics (psychogenic often unrelieved)
- Associated: vomiting, vision change, nasal discharge
- Psychological factors: anxiety, depression
14. Joint Pain
- Age at onset
- First joint affected
- Sequence of involvement
- Persistence or shifting pain
- Swelling or redness?
- Pain with movement?
- Morning stiffness?
- Past trauma?
- Associated: fever, urinary, bowel, or eye issues