Welcome to the Prostate Volume Calculator tool — a simple and accurate way to estimate your prostate gland size and compute your PSA density (PSAD). This online calculator uses clinically accepted formulas to convert your measured prostate dimensions into volume (in cc) and calculates PSA per volume, which is useful in prostate health assessment.
Prostate Volume Calculator
Explore more heart calculator:
The prostate gland is central to male reproductive health. Its size can influence lower urinary tract symptoms, benign prostatic hyperplasia (BPH) and prostate cancer risk. Clinicians often need a quick estimate of gland size to inform decisions such as surveillance, biopsy or treatment planning. A prostate volume calculator converts basic imaging measurements into an estimated volume and, when combined with prostate‑specific antigen (PSA) values, yields the PSA density (PSAD).
Volume estimation is typically derived from ultrasound or magnetic resonance imaging (MRI) measurements. These modalities provide three orthogonal dimensions of the gland, which can be plugged into a geometric formula. While several volumetric models exist, the ellipsoid formula is the most widely accepted in clinical practice. This article explains how the calculator works, why prostate volume matters, how to interpret PSAD, and answers common questions about prostate volume estimation in ultrasound, MRI and computed tomography (CT). The goal is to create a resource that is easy to read yet comprehensive for clinicians, students and patients seeking to understand prostate volumetrics.
Why Prostate Volume Matters
- BPH management – Prostate enlargement can obstruct urinary flow. Knowing the volume helps decide whether medical therapy, minimally invasive procedures or surgery is appropriate. Larger glands may respond less to medication and require surgical intervention.
- Cancer risk assessment – PSA is produced by prostate tissue, so the amount of glandular tissue influences the absolute PSA level. A man with a large prostate may have a PSA that seems high but is proportionate to gland size. Calculating PSAD (PSA ÷ volume) improves specificity for detecting significant cancer.
- Treatment planning – In brachytherapy, radiation dose and seed placement are determined by gland volume. Similarly, prostate artery embolization and ablative therapies consider volume to plan access and dose.
- Monitoring disease – Tracking volume over time helps detect progression of BPH or changes after treatment. Combined with PSA trends, it informs whether a rising PSA is due to growth, inflammation or malignancy.
Understanding the Ellipsoid Formula
The prostate is commonly approximated as a three‑dimensional ellipsoid. The ellipsoid volume formula is: Length × Width × Height × (5π/24) and may be more accurate in some cases.
where the coefficient 0.52 is derived from π/6 and simplifies the classic ellipsoid equation. Most clinical calculators adopt this formula because it is reproducible, quick to apply and aligns with ultrasound and MRI measurement protocols. The prolate ellipsoid model assumes the longest dimension is along the superior–inferior (longitudinal) axis; width is measured transversely, and height (anteroposterior) is measured perpendicular to both.
Alternative Volume Models
Although the ellipsoid formula is dominant, other models may be useful:
- Bullet-shaped formula accounts for prostate asymmetry by modeling the gland as a combination of a cylinder and part of an ellipsoid. Prostate volume is calculated using the formula Length × Width × Height × (5π/24). Some studies suggest this model may better represent prostate shape in selected cases.
- Manual segmentation on MRI – A radiologist outlines the gland on each MRI slice and calculates a true volumetric count. This offers high accuracy but is time‑consuming and requires specialized software.
- 3D ultrasound volumetrics – Some research settings use 3D ultrasound to reconstruct the gland volume; however, it is not widely available.
Even with alternative models, the ellipsoid formula remains the gold standard for routine clinical use because it provides a balance between simplicity and acceptable accuracy.
How to Calculate Prostate Volume
- Obtain imaging measurements – On ultrasound or MRI, measure the maximal prostate dimensions:
- Length – cranio‑caudal dimension (superior to inferior).
- Width – left‑to‑right dimension (transverse).
- Height – anterior‑posterior dimension.
- Convert units – Ensure all measurements are in centimetres (cm). If they are in millimetres (mm), divide by 10.
- Apply the formula – Multiply length × width × height × 0.52 to get the volume in cubic centimetres (cc).
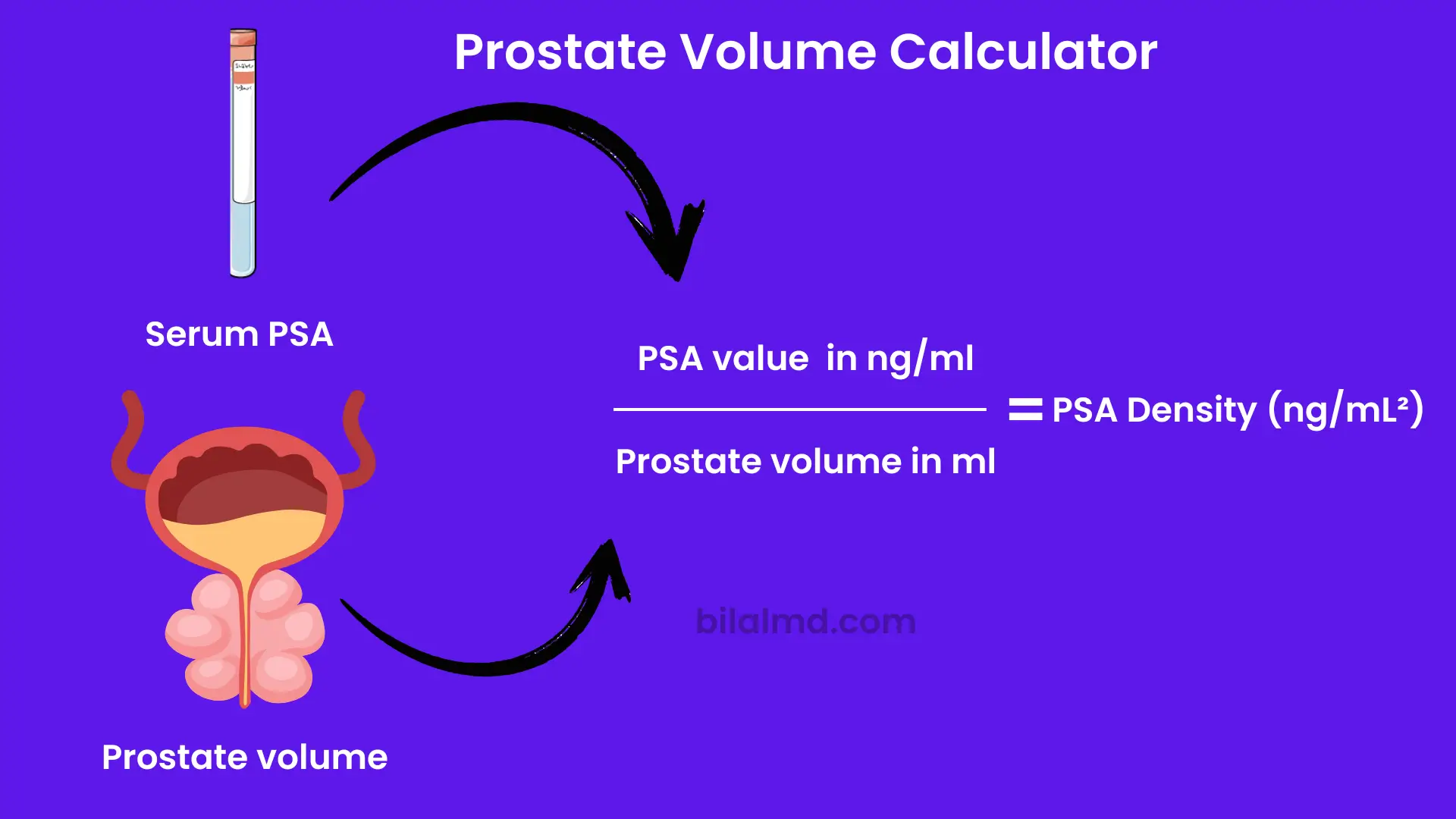
- Calculate PSA density – Divide the patient’s PSA value (ng/mL) by the volume (cc).
For example, a gland measuring 4.8 cm × 4.1 cm × 3.0 cm has a volume:
If the prostate measures 4.8 cm × 4.1 cm × 3.0 cm, the estimated volume is calculated as: Volume = 4.8 × 4.1 × 3.0 × 0.52 = 30.7 cc.
If the PSA level is 6.0 ng/mL, the PSA density (PSAD) is: PSAD = 6.0 ÷ 30.7 ≈ 0.196 ng/mL/cc.
Step‑by‑Step Guide for Clinical Use
- Choose the imaging modality – Ultrasound is widely available and inexpensive but may underestimate volume compared with MRI. MRI provides superior soft‑tissue contrast and correlates better with surgical specimens. CT can also be used but is generally less accurate due to poor soft‑tissue contrast.
- Measure dimensions carefully – In ultrasound, use transverse and sagittal planes. In MRI, measure width on axial T2 images and length and height on mid‑sagittal images.
- Plug into the calculator – Enter your measurements and PSA into an online prostate volume calculator. The tool should display volume (cc) and PSAD.
- Interpret PSAD – Compare the result to clinically relevant thresholds (see below). Lower PSAD values often indicate benign enlargement, while higher values may signal malignancy or the need for further investigation.
- Review limitations – Remember that measurement error, patient factors (e.g., inflammation, ejaculation) and equipment differences can affect the result.
Imaging Modalities: Ultrasound vs. MRI vs. CT
Transrectal ultrasound (TRUS) is the most common method for prostate measurement. It is quick, low‑cost and can be performed in an outpatient setting. However, TRUS measurements may be less accurate in larger prostates or when median lobes protrude into the bladder. In a study of 318 patients who had both TRUS and MRI prior to radical prostatectomy, MRI volume estimates showed better correlation with specimen volume (interclass correlation 0.83 vs. 0.74 for TRUS). TRUS volumes differed by more than 10 cc from pathology in 29% of cases compared with 23% for MRI.
MRI offers superior spatial resolution and contrast, allowing more accurate delineation of prostate margins. It tends to slightly overestimate volume but is particularly useful when TRUS and MRI estimates disagree. MRI is often employed in active surveillance programs and pre‑biopsy assessments, where precise volume measurement influences risk stratification and treatment planning.
CT can estimate prostate size, especially in emergency or non‑urologic imaging; however, its lower soft‑tissue contrast makes measurements less reliable. CT should not be used as the primary modality for volume estimation when ultrasound or MRI is available.
Understanding PSA Density (PSAD)
PSA density normalizes PSA levels by the size of the gland. It is calculated by dividing PSA (ng/mL) by prostate volume (cc). PSAD is particularly useful when PSA values fall in the “gray zone” (4–10 ng/mL). A man with a large prostate may have an elevated PSA because of benign hyperplasia; dividing by volume yields a lower PSAD, suggesting benign disease. Conversely, a small prostate with elevated PSA leads to a high PSAD and greater suspicion of malignancy.
Interpreting PSAD Thresholds
- 0.10–0.15 ng/mL/cc – Historically used thresholds. Many studies and guidelines reference a PSAD cutoff around 0.15 ng/mL/cc for recommending prostate biopsy. This threshold is mentioned in several European Association of Urology (EAU) guidelines and has been widely adopted in clinical practice.
- 0.08–0.15 ng/mL/cc – Some calculators note that universal cut‑off values are not established and that suggested cut‑offs range from 0.08 to 0.15 depending on PSA level, imaging quality and individual factors.
- ≥0.20 ng/mL/cc – Recent research questions the traditional 0.15 threshold. A study assessing the justification for the 0.15 cut‑off found no clear change in risk at that value; the probability of high‑grade cancer associated with PSAD 0.15 ranged from 2.6% to 10%. The authors suggest a threshold of at least 0.20 ng/mL/cc, particularly when MRI quality is adequate.
- Personalization – Some clinicians adjust the threshold based on patient age, race, body mass index, digital rectal examination findings and family history. The threshold may also differ based on whether MRI or TRUS measurements are used.
A PSAD above the chosen threshold does not necessarily indicate cancer but suggests a higher risk warranting further evaluation, such as MRI, repeat PSA testing or biopsy.
Limitations and Considerations
While calculators provide useful estimates, their accuracy is influenced by several factors:
- Measurement error – Small errors in measuring length, width or height can lead to significant differences in calculated volume. Image quality, probe positioning and operator experience play critical roles.
- Prostate shape variation – Glands are rarely perfect ellipsoids. Irregular shapes, nodules or asymmetry can cause the ellipsoid formula to underestimate or overestimate the true volume. In such cases, the bullet formula or manual segmentation may provide better approximations.
- Imaging modality differences – TRUS often underestimates large prostates compared with MRI. CT may overestimate because of poorer soft‑tissue contrast. When TRUS and MRI measurements differ, MRI may be more reliable.
- PSA fluctuations – PSA can be elevated by prostatitis, recent ejaculation, urinary retention, catheterization or instrumentation. Always interpret PSAD in conjunction with clinical history and other diagnostic tests.
- Threshold variability – PSAD cutoffs are not universally standardized. Different guidelines and studies propose thresholds ranging from 0.10 to 0.20 ng/mL/cc. Clinicians should consider patient‑specific factors and imaging quality when applying thresholds.
Frequently Asked Questions
How to calculate prostate volume?
To calculate prostate volume, multiply the length, width and height of the gland (in centimetres) and then multiply by 0.52. This assumes an ellipsoid shape.
How do you calculate prostate volume in ultrasound?
Transrectal ultrasound (TRUS) measurements require careful placement of the probe. Measure the three orthogonal dimensions in the sagittal and transverse planes, convert to centimetres and apply the ellipsoid formula. Note that TRUS may underestimate volume compared with MRI.
How to calculate prostate volume by ultrasound?
Use TRUS to acquire length, width and height. Multiply the measurements by 0.52. Some clinicians may apply a correction factor or use bullet models when TRUS underestimates volume in large glands.
How to calculate prostate volume on CT or MRI?
On MRI, measure width on axial T2 images and length and height on mid‑sagittal T2 images. MRI is generally more accurate than TRUS and may overestimate slightly. CT measurements follow the same principle but are less reliable due to poorer soft‑tissue differentiation.
Why use a prostate gland volume calculator?
A calculator standardizes the conversion of imaging measurements into volume. It reduces manual errors and automatically computes PSA density when PSA is entered. This aids clinicians in quick risk assessment and patient counselling.
How to interpret PSA density?
Divide PSA by prostate volume to obtain PSAD. Compare the result to thresholds (0.10–0.20 ng/mL/cc). A low PSAD suggests PSA elevation due to benign tissue; a higher PSAD suggests higher cancer risk.
Is the 0.15 ng/mL/cc threshold still valid?
The 0.15 ng/mL/cc cut‑off is widely referenced in guidelines. However, recent analysis suggests that this threshold may not correspond to a marked increase in cancer risk; thresholds of 0.20 ng/mL/cc or individualized cut‑offs may be more appropriate.
How accurate is prostate volume measurement?
Accuracy depends on modality. MRI correlates more closely with surgical specimens than TRUS. Ultrasound is operator dependent and may underestimate large prostates or those with median lobes. Even MRI can slightly overestimate volume in some cases.
Can I use digital rectal exam to estimate prostate volume?
Digital rectal examination (DRE) provides only a rough estimate and is not accurate enough to calculate PSAD. Imaging measurements are essential.
What if my PSA is high but PSAD is low?
A high PSA with low PSAD often indicates benign enlargement rather than cancer. Your clinician may recommend continued surveillance or medical management rather than immediate biopsy.
Can the prostate volume calculator diagnose cancer?
No. The calculator is a screening tool. Diagnosis of prostate cancer requires histologic confirmation via biopsy. The calculator helps identify those who may need further evaluation but should not replace clinical judgement.
How often should prostate volume be measured?
For patients on active surveillance or with BPH, volume may be assessed annually or during routine PSA testing. Frequency depends on symptoms, PSA trends and treatment status.
Conclusion
Prostate volume estimation and PSA density calculation are valuable tools in urologic practice. The ellipsoid formula remains the cornerstone for calculating volume, offering a simple and reproducible method. Alternative models such as bullet‑shaped volume and manual segmentation exist, but they are used less frequently due to complexity.
While a prostate volume calculator provides convenience, clinicians must be aware of its limitations. Differences between ultrasound and MRI, variability in measurement and the lack of a universal PSAD threshold mean that results must be interpreted in context. Emerging evidence suggests that the traditional PSAD cut‑off of 0.15 ng/mL/cc may be too low, with new studies recommending thresholds of 0.20 ng/mL/cc or personalized cut‑offs.
Ultimately, prostate volume and PSA density should be integrated with patient history, digital rectal examination, MRI findings and other biomarkers. By using these calculators judiciously, clinicians can improve risk stratification, reduce unnecessary biopsies and tailor management strategies to individual patients, enhancing the quality and precision of prostate care.