During my house job, I often faced confusion when managing hypernatremia and trying to quickly estimate how much “free water” a patient actually needed. Even when the formula was known, converting sodium values into a practical deficit number and then planning safe correction could feel stressful in a busy ward. This Free Water Deficit Calculator is made to simplify that process by giving you a clear estimate of free water deficit based on standard inputs, so you can move from lab values to a practical clinical plan faster and with more confidence.
Free Water Deficit Calculator
Estimate free water deficit for hypernatremia using standard TBW formulas.
Want deeper teaching examples and a printable reference? See our companion guide.
Explore more nephrology calculators:
What is “free water deficit”?
Free water deficit is the estimated volume of electrolyte-free water a patient needs to return an elevated serum sodium (hypernatremia) toward normal. It’s a practical way to translate a lab value into an actionable fluid plan, especially when hypernatremia reflects net water loss from fever, diuresis, diarrhea, or diabetes insipidus.
The standard free water deficit formula (and TBW multipliers)
Most bedside references use the same core equation:
Free Water Deficit (L) = TBW × [(Measured Na⁺ / 140) − 1]

Where TBW (total body water) is estimated from weight and a sex/age factor:
- Adult male: 0.6 × weight (kg)
- Adult female: 0.5 × weight (kg)
- Elderly male: 0.5 × weight (kg)
- Elderly female: 0.45 × weight (kg)
These factors and the 140 mEq/L “target” sodium are widely cited in clinical references and calculators.
Pro tip: In markedly water-depleted or low-lean-mass patients, many clinicians use slightly lower TBW fractions (e.g., ~0.5 men, ~0.4 women) to avoid underestimating the deficit.
How to calculate free water deficit (step-by-step)
- Confirm hypernatremia and its likely duration (acute <48 h vs chronic/unknown). This determines how fast you’ll correct.
- Estimate TBW: multiply weight (kg) by the appropriate factor above.
- Apply the formula: TBW × [(Na⁺/140) − 1]. The result is liters of electrolyte-free water needed to move Na⁺ toward 140 mEq/L.
- Plan delivery & rate: Replace over 48–72 hours in most chronic cases, adjusting for ongoing losses (fever, polyuria, stool).
- Choose a fluid: Typical options are D5W (5% dextrose in water) or 0.45% saline, or oral water if safe. Resuscitate shock first with isotonic fluid.
Worked example (for illustration)
- 70-kg adult male with Na⁺ 160 mEq/L
- Deficit = 42 × [(160/140) − 1] = 42 × (1.1429 − 1) ≈ 6.0 L
A reasonable plan is to replace ~6 L of free water plus ongoing losses over 2–3 days, monitoring sodium every 2–4 hours initially and adjusting as needed.
Safe correction targets
- Chronic or unknown duration: aim to lower Na⁺ by ≤0.5 mEq/L per hour and ~6–12 mEq/L in the first 24 hours; complete the calculated replacement over 48–72 hours. Faster correction risks cerebral edema.
- Acute (<48 h) symptomatic sodium gain: can initially correct faster (~1–2 mEq/L per hour for 6–8 h) toward 145 mEq/L if clinically appropriate, then slow.
- Practical note: Recent adult data suggest that very slow correction may be associated with higher mortality; if you inadvertently slightly exceed the target rate, re-raising sodium is generally not recommended. Use clinical judgment and close monitoring.
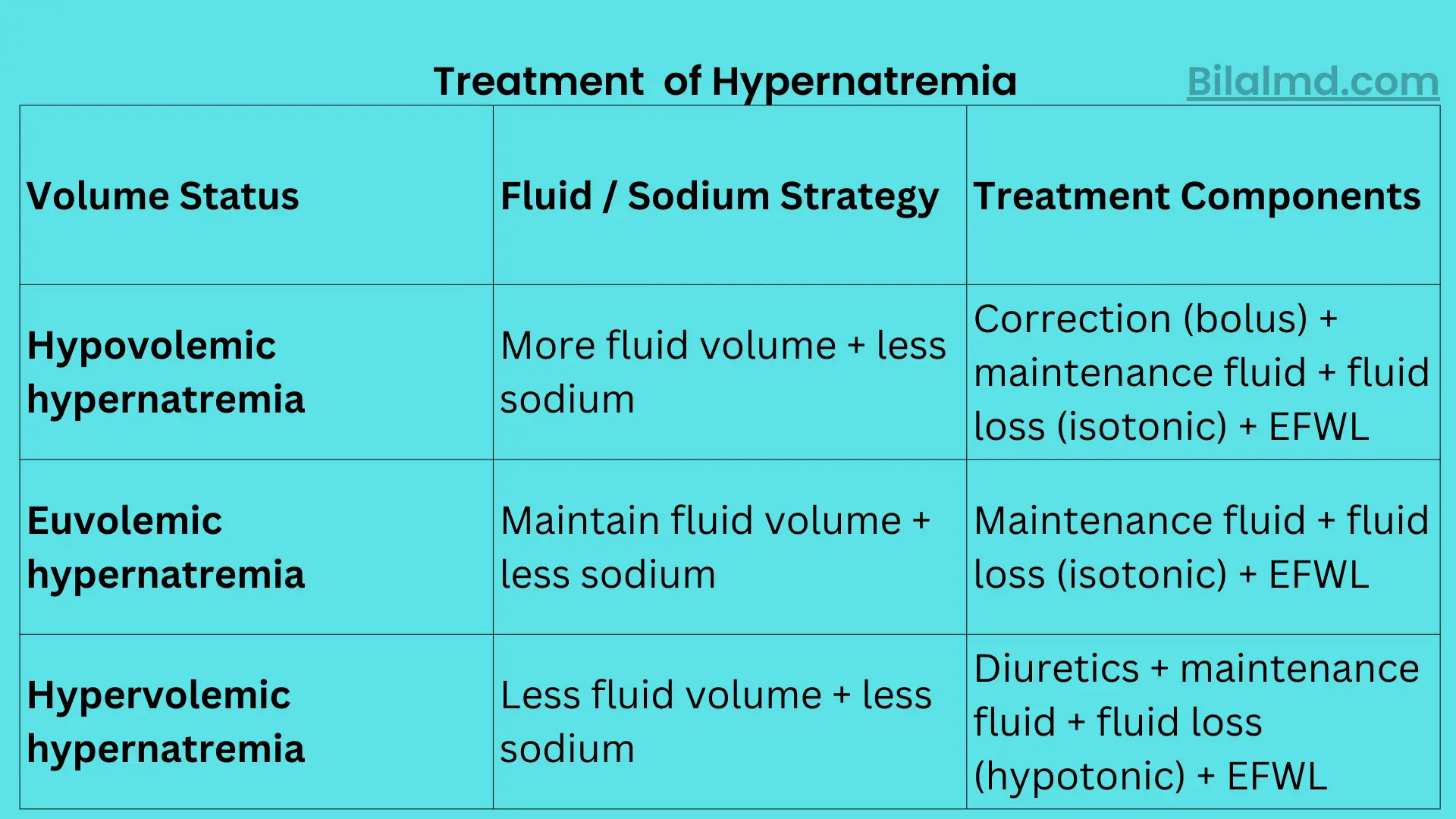
Choosing fluids & accounting for ongoing losses
- Start with isotonic fluid if the patient is hypovolemic/shocky, then switch to hypotonic replacement for the deficit.
- For the free water portion, D5W (IV) or 0.45% saline (IV) are commonly used; oral water works if safe. Always add insensible and ongoing renal/GI losses to the plan.
- In massive sodium loading or volume-overloaded states, you may need loop diuretics or even dialysis alongside free water.
Common pitfalls
- Forgetting TBW differences: Using the wrong TBW factor can under- or over-estimate the deficit. Our calculator applies the standard factors and lets you adjust for age/sex.
- Ignoring duration: Correction targets depend on acute vs chronic; the risk profile is different.
- Not adding ongoing losses: Polyuria (DI), diarrhea, fever, or drains can erase your gains; track outputs and re-calculate.
- Failing to monitor: Check serum sodium every 2–4 hours at the start and adjust fluid rates accordingly.
FAQs For free water feficit calculator
How to calculate free water deficit?
Use: TBW × [(Measured Na⁺ / 140) − 1]. Estimate TBW from weight using 0.6 (adult men), 0.5 (adult women), 0.5 (elderly men), 0.45 (elderly women). Then plan replacement over 48–72 hours in chronic cases.
How do you calculate free water deficit in hypernatremia?
Exactly as above; the formula is designed for hypernatremia. After you compute the liters of electrolyte-free water, choose D5W or 0.45% saline (or oral water), add ongoing losses, and monitor sodium closely.
How to calculate water deficit in dehydration?
Dehydration is a common cause of hypernatremia. Use the same free water deficit equation and add replacement for volume depletion (initial isotonic fluid if needed) before hypotonic water replacement.
Calculating free water deficit vs “electrolyte-free water clearance” what’s the difference?
The deficit estimates how much water to give to reach a target sodium. Electrolyte-free water clearance is a urinary calculation that helps quantify ongoing renal losses; it’s useful but impractical for routine bedside use.
How to calculate free water deficit if the patient is obese or severely water-depleted?
Many clinicians lower the TBW fraction (e.g., ~0.5 for men, ~0.4 for women, or use lean body weight) so you don’t underestimate the deficit. Always pair the estimate with clinical monitoring and frequent labs.
Why use our calculator and where to go next
- Fast & focused: Enter weight and sodium, pick the TBW factor, and you’ll get a precision estimate in seconds.
- Clinically aligned: Mirrors the equation and factors recommended in major references, so you can trust the math.
- Learn as you go: Our blog regularly publishes practical, non-jargon guides on fluids, electrolytes, acid-base, and nephrology. Use the calculator here, then hop to the blog for deeper case-based learning and from the blog, jump right back to this calculator when you need it most.
Quick safety checklist before you start fluids
- Confirm acute vs chronic onset and assess volume status.
- If in shock/hypovolemia, start with isotonic fluid.
- Target ≤0.5 mEq/L/hr (6–12 per day) in chronic/unknown cases; consider faster initial rates only in acute symptomatic sodium gain.
- Re-check sodium every 2–4 hours, watch neurologic status, and adjust the plan.