A STEMI Calculator helps clinicians move faster and think clearer when every minute counts. It guides diagnosis when the electrocardiogram is not straightforward, estimates a patient’s short term risk, and supports the choice and timing of reperfusion. Used well, a STEMI Calculator does not replace judgment. It accelerates good judgment with structured inputs and validated scores.
STEMI Calculator – TIMI Risk Score
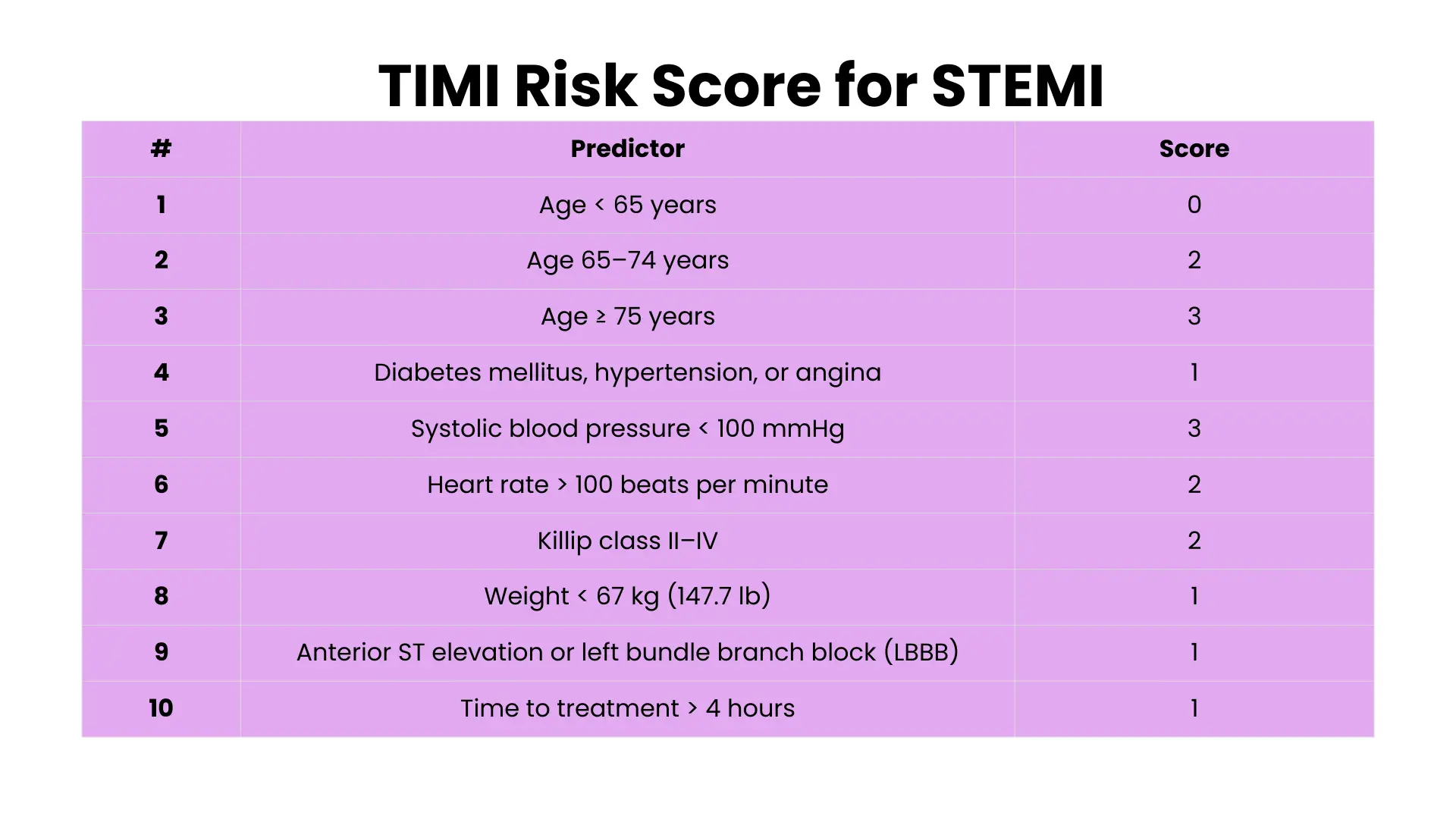
Estimates 30-day mortality at presentation for ST-elevation MI (TIMI STEMI). Select applicable items then press Calculate. Score range: 0 – ≥9
Disclaimer & sources
This tool is for education / decision support. It does not replace judgment or cardiology consult.
- Morrow et al. TIMI risk score for STEMI. Circulation 2000.
- TIMI Risk Score for STEMI (official).
- 30-day mortality table (Merck Manual).
- Door-to-balloon ≤90 min, door-to-needle ≤30 min (NEJM review).
Explore more heart calculator:
First principles what counts as STEMI
ST elevation myocardial infarction is myocardial injury from acute coronary artery occlusion with characteristic electrocardiographic changes and a rise and fall in cardiac troponin. The Fourth Universal Definition of Myocardial Infarction sets the biomarker standard and clarifies that a dynamic change in cardiac troponin above the ninety ninth percentile defines acute injury in the right clinical context.
Electrocardiographic criteria are precise. ST elevation is measured at the J point in two contiguous leads with sex and age specific thresholds in the anterior leads and a one millimeter threshold in other leads. Contemporary summaries list at least two and a half millimeters in V2 or V3 for younger men, two millimeters in V2 or V3 for older men, one and a half millimeters in V2 or V3 for women, and one millimeter in any other contiguous leads. These thresholds are paired with recognition of STEMI equivalents including posterior infarction, de Winter pattern and Wellens changes which demand urgent reperfusion.
Time targets guide care. Systems of care aim for door to balloon within ninety minutes for primary percutaneous coronary intervention and door to needle within thirty minutes for in hospital fibrinolysis when percutaneous coronary intervention is not immediately available. Faster treatment improves outcomes.
What a STEMI Calculator actually calculates
There is not one single STEMI Calculator. The term covers three useful families of tools.
Diagnostic calculators
These help when the electrocardiogram is hard to interpret. The classic problem is left bundle branch block where baseline ST changes mask ischemia. The Sgarbossa criteria and the modified Sgarbossa rule by Smith improve detection of occlusion in left bundle branch block by scoring concordant and excessively discordant ST deviation. Most clinicians access these rules through point of care tools like MDCalc. Used correctly they flag probable occlusion that warrants immediate invasive management.
There are also calculators for subtle anterior infarction that combine measured ST elevation in specific anterior leads with reciprocal changes to raise suspicion when the tracing looks almost normal. These do not replace serial electrocardiograms or clinical assessment. They push you to repeat an electrocardiogram, obtain posterior or right sided leads, and involve cardiology early when the score is concerning.
Risk and prognosis calculators
Risk calculators answer a different question. Once you confirm or strongly suspect ST elevation myocardial infarction, what is the early risk of death or shock. The TIMI risk score for STEMI is a simple bedside score validated to predict thirty day mortality. It assigns points for age, past history of diabetes or hypertension or angina, low systolic pressure, high heart rate, Killip class, low body weight, anterior infarction or left bundle branch block, and delay to treatment beyond four hours. Higher total points correlate with sharply higher mortality.
The GRACE score estimates in hospital and six month mortality in acute coronary syndromes using age, vital signs, creatinine, cardiac arrest at admission, Killip class, cardiac enzymes, and ST segment deviation. It often complements TIMI because it includes renal function and a broader set of clinical variables. Both are accessible as bedside calculators.
An even more rapid option is the TIMI Risk Index which uses only age, heart rate, and systolic pressure to give an initial mortality estimate before full labs return.
System and quality timers
You will not see a field labeled door to balloon inside a typical STEMI Calculator, yet time metrics are the silent backbone behind these tools. The goal is first medical contact to device within ninety minutes for primary percutaneous coronary intervention. When this cannot be achieved, fibrinolysis should begin within thirty minutes and transfer to a percutaneous coronary intervention center should follow without delay. A good calculator keeps you focused on these clocks by reminding you the moment you enter symptom onset time or first medical contact time.
How to use a STEMI Calculator step by step
Step one decide what you need to know
If the tracing is obvious with clear ST elevation in contiguous leads and the patient has ischemic symptoms, do not delay reperfusion to hunt for a score. Activate the catheterization team or give fibrinolytics according to your local pathway. Calculators add value when the tracing is equivocal, when left bundle branch block or ventricular paced rhythm limits interpretation, or when you must estimate risk to guide triage and intensity of monitoring.
Step two enter clean data
For a diagnostic rule in left bundle branch block measure the millimeters of ST deviation at the J point and note whether the deviation is concordant or discordant relative to the QRS complex. For TIMI or GRACE ensure you have an accurate heart rate and blood pressure, Killip class, weight if needed, and initial troponin status. Small errors in these inputs will swing the risk estimate in the wrong direction.
Step three interpret and act
A positive modified Sgarbossa rule in a patient with ischemic symptoms justifies immediate reperfusion as an occlusion myocardial infarction equivalent. A high TIMI risk score should push you toward intensive monitoring, early invasive strategy, shock team readiness, and careful anticoagulation and antiplatelet planning. A high GRACE score supports early transfer if you are in a facility without percutaneous coronary intervention capability. None of these scores replace clinical assessment or serial electrocardiograms. They refine the probability and communicate risk to the team in a shared language.
When a STEMI Calculator changes decisions
Consider a patient with chest pressure and left bundle branch block on the electrocardiogram. The tracing shows one millimeter of ST elevation in a lead with a positive QRS and five millimeters of discordant elevation in a lead with a negative QRS. A modified Sgarbossa score would be positive, which should prompt activation for emergent percutaneous coronary intervention even if the troponin has not yet resulted. In another case with classic anterior ST elevation and hypotension, a TIMI risk score that lands in a high range reminds the team to anticipate shock, to place arterial access early, and to consider mechanical support as needed.
Limitations you should respect
A STEMI Calculator is only as good as the measurements you feed it. Misread ST segments, wrong heart rate, or misclassified Killip class will mislead you. Scores predict risk, they do not diagnose infarction on their own. Diagnostic rules that aid interpretation in left bundle branch block can still miss early posterior infarction or subtle high lateral injury. Always repeat electrocardiograms, look for reciprocal changes, and correlate with the story and exam. Universal definition principles still apply. You need a compatible clinical picture and evidence of acute myocardial injury, not just a number on a screen.
Building or choosing a STEMI Calculator for your site or service
If you are creating a STEMI Calculator for a website or a local pathway, include three modules. First, a diagnostic helper with modified Sgarbossa and a simple subtle anterior tool. Second, a risk tab with TIMI for STEMI, GRACE, and the TIMI Risk Index for fast triage. Third, a timer widget that tracks first medical contact to device and door to needle. Link each output to clear next steps such as activate the catheterization team, consider fibrinolysis and transfer, or escalate monitoring. Include plain language reminders that scores assist but do not replace judgment. Finally, default your labels to the same thresholds used in current American and European guidance so your numbers match what cardiology expects.
Frequently asked questions about STEMI Calculator
Can a STEMI Calculator diagnose a heart attack by itself
No. Diagnosis rests on symptoms, electrocardiogram changes, and dynamic troponin. Calculators support these decisions but do not stand alone. Follow the universal definition and your local protocol.
Which risk score should I use first in the emergency department
Start with TIMI for STEMI because it uses data available at the bedside and predicts thirty day mortality. Add GRACE when you have labs and want an in hospital or six month estimate that includes renal function and Killip class.
How do I handle left bundle branch block
Use the modified Sgarbossa rule. A positive result in a patient with ischemic symptoms is an occlusion equivalent and should prompt urgent reperfusion without delay.
What time targets should my team track
Aim for door to balloon within ninety minutes for primary percutaneous coronary intervention. If transfer will delay beyond that window, give fibrinolysis within thirty minutes and transfer promptly.
Do sex and age change the amount of ST elevation needed
Yes in the anterior precordial leads V2 and V3 the cutoffs vary by sex and age, while in other contiguous leads one millimeter is sufficient. Use the published thresholds and always read the tracing in clinical context.
Is there any benefit to the TIMI Risk Index when I am very busy
Yes. It uses only age, heart rate, and systolic pressure to give a rapid mortality estimate before labs return. It does not replace fuller scores but it is fast and practical.
Can I use a STEMI Calculator in the field
Yes. Prehospital use of risk scores and diagnostic rules can prompt earlier activation of the catheterization team and shave minutes off door to balloon. Integrate the tool into your first medical contact workflow, do not let it slow patient transfer.
Bottom line
A STEMI Calculator is a practical companion for emergency clinicians and prehospital teams. It helps identify occlusion when the tracing is complex, it quantifies early risk so you can plan care, and it keeps attention on the clocks that save myocardium. Use diagnostic rules like modified Sgarbossa when the baseline electrocardiogram is hard to read. Use TIMI, GRACE, and the TIMI Risk Index to stratify risk and to communicate it clearly. Above all, treat the patient first and let the calculator make a good decision faster.