An RCRI calculator gives you a quick, evidence-based estimate of a patient’s risk of major cardiac complications before noncardiac surgery. If you need a lightweight, bedside tool that’s simple, transparent, and validated, this is it. The Revised Cardiac Risk Index (RCRI) has six equally weighted predictors and a 0–6 score that maps to event rates commonly cited in practice (≈0.4%, 0.9%, 6.6%, and ≥11%). It’s not magic; it’s a pragmatic signal you combine with clinical judgment and contemporary guideline steps.
RCRI Calculator – Revised Cardiac Risk Index
Estimate risk of major cardiac complications after noncardiac surgery.
Select risk factors (1 point each)
Medical Disclaimer
This calculator is provided for educational and informational purposes only. It does not provide medical advice, diagnosis, or treatment and must not be used as a substitute for professional clinical judgment. Clinical decisions should always be made by qualified healthcare professionals based on the individual patient’s condition, medical history, and current clinical guidelines.
Explore more heart calculator:
What is the RCRI and why should you care?
The Revised Cardiac Risk Index (RCRI), derived by Lee et al. in 1999, is a six-predictor model that estimates the risk of major cardiac complications (e.g., myocardial infarction, pulmonary edema, ventricular fibrillation/primary cardiac arrest, complete heart block) after noncardiac surgery. It was built as a revision of Goldman’s index and became popular because it’s fast, reproducible, and easy to remember.
In 2024, the AHA/ACC perioperative guideline again endorsed a stepwise approach and explicitly named validated risk tools like the RCRI and ACS NSQIP as useful inputs to decision-making not as substitutes for judgment. Translation: use an RCRI risk calculator alongside functional status, surgical urgency, and risk modifiers.
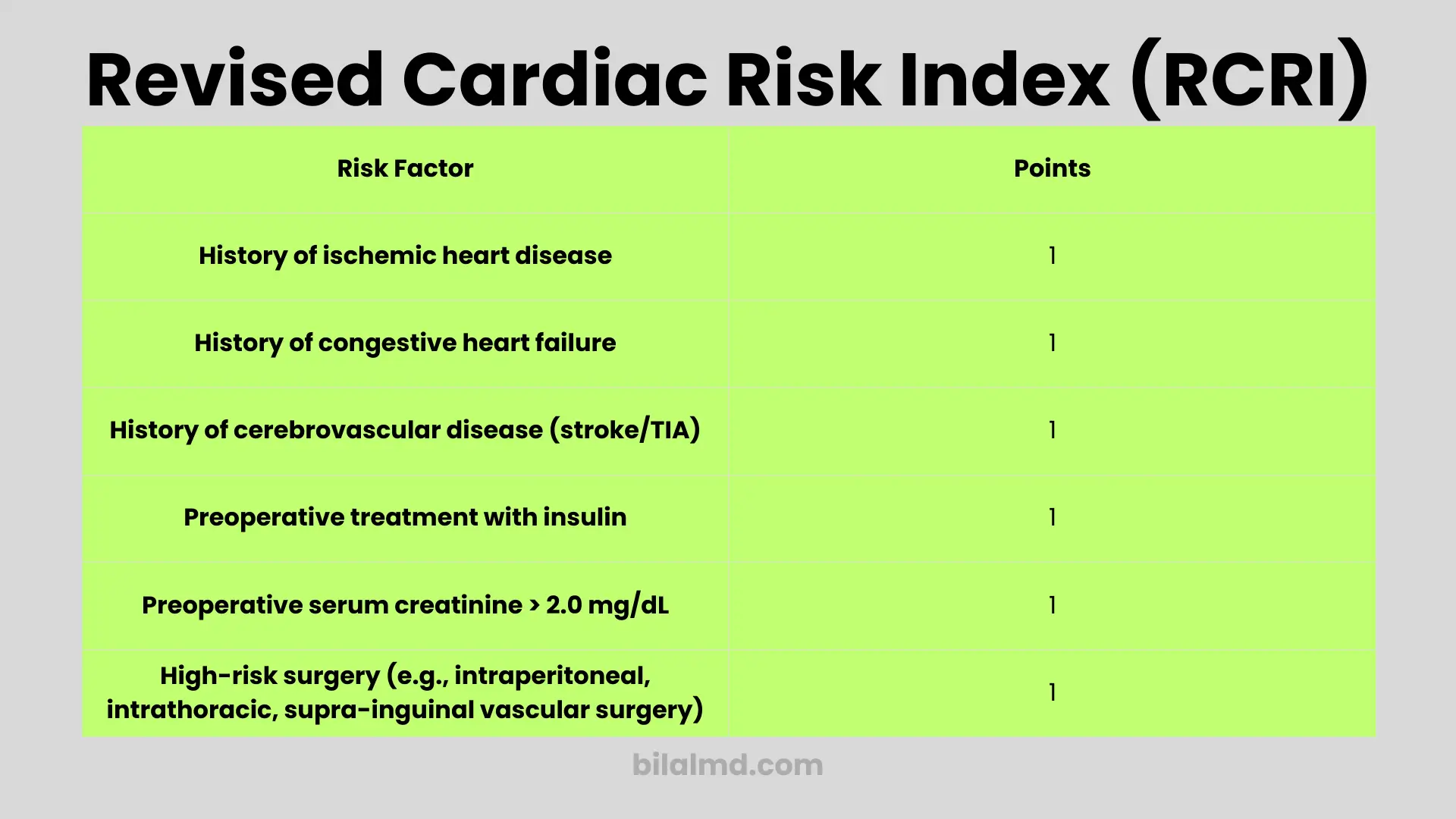
The six RCRI predictors (1 point each)
Add one point for each predictor present pre-op:
- High-risk surgery (intraperitoneal, intrathoracic, or suprainguinal vascular).
- History of ischemic heart disease.
- History of congestive heart failure.
- History of cerebrovascular disease (stroke/TIA).
- Insulin-treated diabetes mellitus.
- Pre-op serum creatinine > 2.0 mg/dL (≈177 µmol/L).
These are binary no partial credit, no weighting games. That simplicity is the point: the RCRI score calculator you use at the bedside is literally a 0–6 count.
How to calculate RCRI in under 30 seconds
If you’re looking to calculate RCRI fast, use this workflow:
- Confirm the surgery category. If it’s intraperitoneal, intrathoracic, or suprainguinal vascular, add 1 for high-risk surgery.
- Scan the problem list/history: IHD, CHF, CVA/TIA, insulin-treated DM add 1 for each present.
- Check creatinine; if it’s > 2.0 mg/dL (≈177 µmol/L), add 1.
- Sum the points (0–6). That’s the RCRI calculation.
Interpreting the score (what the numbers actually mean)
Event rates commonly cited in clinical references and calculators map roughly like this:
- Score 0 → ~0.4%
- Score 1 → ~0.9%
- Score 2 → ~6.6%
- Score ≥3 → ≥11%
These figures trace to the derivation/validation data and are reproduced across trusted calculators used by clinicians. Don’t pretend they’re perfect predictions for every subpopulation; treat them as risk bins that inform your bigger pre-op picture.
When (and when not) to use an RCRI risk calculator
Use it when:
- You need a transparent baseline estimate during pre-op for noncardiac surgery.
- You’re following the 2024 AHA/ACC stepwise process and want a validated tool alongside clinical assessment.
Don’t rely on it alone when:
- A nuanced, patient-specific question calls for procedure-specific outcomes (wound, pneumonia, renal failure, etc.) this is where ACS NSQIP shines with broader endpoints and surgical CPT context.
- You’re evaluating special cohorts where RCRI performance varies (e.g., certain vascular cases, pararenal aneurysm surgery). The literature shows heterogeneous calibration in subgroups.
RCRI vs. other tools (ACS NSQIP MICA, etc.)
- RCRI is simple (6 yes/no items), fast, and interpretable at the bedside even with no computer.
- ACS NSQIP calculators (e.g., MICA) ingest more variables and aim at procedure-specific risks, sometimes offering better discrimination but at the cost of complexity. Head-to-head studies have shown mixed comparative performance by endpoint and cohort; that’s fine use the right tool for the right question.
Practical approach: start with the RCRI score calculator to frame the cardiac piece, then, if decisions hinge on finer-grained risk or non-cardiac outcomes, run NSQIP as well. This approach aligns with the 2024 guideline (validated tools plural).
Don’t forget functional capacity and risk modifiers
A good RCRI calculation is not a license to ignore the basics. Two reality checks you should always include:
- Functional capacity (METs): poor capacity ups risk and can change testing/optimization steps. Even the best calculator is blunt if the patient can’t climb a flight of stairs without symptoms.
- Clinical modifiers: active cardiac conditions, unstable symptoms, or recent coronary events trump any calculator and should trigger evaluation per guideline.
Step-by-step example (walkthrough)
Say your patient is scheduled for an open intraperitoneal resection, has prior MI, no CHF, no stroke/TIA, is on insulin, and creatinine is 2.3 mg/dL.
- High-risk surgery → +1
- IHD → +1
- CHF → 0
- CVA/TIA → 0
- Insulin-treated DM → +1
- Creatinine > 2.0 mg/dL → +1
Total: 4 points → You’re in the ≥11% bin. That pushes you to a serious conversation about timing, optimization, monitoring, and peri-op strategy, potentially including cardiology input exactly what the 2024 AHA/ACC stepwise approach is designed to systematize.
Strengths, limitations, and honest caveats
Strengths
- Speed & simplicity: six yes/no items, no black box.
- External familiarity: most teams recognize it; you won’t waste time explaining the scale.
- Guideline-compatible: still recommended as a validated tool in modern perioperative workflows.
Limitations
- Not procedure-granular: it won’t tell you pulmonary or wound risks; it’s strictly cardiac complications. Pair it with NSQIP when you need broader endpoints.
- Calibration drift: patient mix and peri-op care have changed since 1999. Contemporary reviews note variable performance across populations; you’re expected to use judgment.
- Edge cases: Some vascular subtypes show weaker predictability with RCRI alone. Don’t be lazy here cross-check with other tools and clinical context.
Bottom line: the RCRI is a good signal, not a verdict.
How to write up the result (so it’s useful)
- “RCRI score 2/6 (Class III) → estimated cardiac event risk ≈6.6%. We also assessed functional capacity, meds, and surgical urgency per 2024 AHA/ACC guidance; plan includes optimization of comorbidities and peri-operative monitoring.”
That one sentence shows you computed the RCRI risk calculator result and put it in a guideline-concordant context.
FAQ
Is RCRI still recommended today?
Yes 2024 AHA/ACC reiterates using validated tools like RCRI and NSQIP in a stepwise pre-op evaluation.
What is the RCRI and when should I use it?
The Revised Cardiac Risk Index is a six-item, yes/no bedside tool that estimates the risk of major cardiac complications after noncardiac surgery. Use it as one input in a stepwise pre-op assessment alongside clinical judgment, functional capacity, and surgical urgency not as a standalone “green light.” The 2024 AHA/ACC perioperative guideline explicitly supports using validated tools like RCRI (and NSQIP) within a structured workflow.
How do I calculate RCRI correctly?
Give 1 point each for: high-risk surgery, history of ischemic heart disease, history of congestive heart failure, history of cerebrovascular disease, insulin-treated diabetes, and creatinine >2.0 mg/dL (≈177 µmol/L). Sum 0–6. That’s it no partial credit, no weights.
What do the RCRI risk bins mean?
Commonly cited event rates: 0 → ~0.4%, 1 → ~0.9%, 2 → ~6.6%, ≥3 → ≥11% for major cardiac events. Treat these as risk categories, not precise predictions for every population.
RCRI vs NSQIP (Gupta/MICA): which should I use?
Use RCRI for a fast, transparent cardiac risk snapshot; use NSQIP/MICA when you need procedure-specific, multi-outcome estimates and better discrimination for certain decisions (it ingests CPT, ASA class, functional status, etc.). In practice, many clinicians start with RCRI and add NSQIP if decisions hinge on finer-grained risk. That’s aligned with 2024 AHA/ACC guidance. Reddit discussions often echo this pragmatic combo.
My RCRI is low should I still get a stress test?
Not automatically. Routine stress testing for low predicted risk or adequate functional capacity isn’t recommended. Consider testing only when results would change management and the patient’s risk/functional status suggests it. This is a recurring confusion in exam-prep threads; follow the stepwise guideline rather than a blanket RCRI threshold.
METs vs RCRI: which matters more?
Both matter. Poor functional capacity (<4 METs) increases concern even when RCRI is low; good functional capacity can reassure when RCRI is borderline. Combine them don’t cherry-pick whichever is lower. This point comes up repeatedly in student and resident threads.
Should I ever write “medically cleared for surgery”?
No. Replace “clearance” language with risk stratification and optimization wording: e.g., “At present, patient is medically optimized to proceed at ~X% estimated 30-day cardiac risk by RCRI; further testing not expected to change management.” This is a common Reddit gripe and it aligns with best practice and medicolegal prudence.
How do I document RCRI risk so the team actually reads it?
State the score and class, the estimated % risk, and what you did or didn’t do (and why). Example: “RCRI 2/6 (Class III) → ~6.6% risk; no active cardiac conditions; <4 METs but testing would not alter management; optimization steps X/Y completed.” Reddit clinicians emphasize dropping “cleared” and giving a succinct, actionable paragraph.
What exactly counts as high-risk surgery in RCRI?
RCRI’s “high-risk surgery” means intraperitoneal, intrathoracic, or supra inguinal vascular procedures. If you’re on the fence for a specific operation, cross-check the surgical approach/category and consider NSQIP for a procedure-specific estimate.
My patient has ECG abnormalities, but RCRI doesn’t care. Now what?
Correct: ECG findings aren’t in RCRI (or NSQIP) inputs. Don’t ignore them evaluate clinically per guideline triggers (symptoms, active cardiac conditions, planned surgery). Use RCRI as one piece of the picture.
When does a high RCRI push you to cardiology?
When the score is ≥3, when functional capacity is poor, when there are active cardiac conditions, or when you foresee management changes (e.g., medication optimization, monitoring level). Reddit threads and the 2024 guideline both steer away from reflex testing and toward targeted optimization.
Is pre-op “clearance” in urgent care a thing?
It shouldn’t be. Risk stratification and optimization require continuity and records; urgent care is a poor setting for that. Reddit consensus is to redirect for proper evaluation and documentation.
Any template or flowsheet you recommend?
Clinicians on Reddit share brief, structured notes: indication, surgery type, RCRI score/%, functional capacity, optimization steps, monitoring plan, plus whether further testing would change management. If you need richer, procedure-specific numbers, add NSQIP.
Who actually makes the go/no-go decision?
Not the PCP alone. The surgeon + anesthesia team own the final decision, informed by your risk stratification and optimization. That’s the consistent message from clinicians in Reddit threads and the team-based model in the guideline.
Are there alternatives or adjuncts to RCRI?
Yes. In addition to NSQIP/MICA, there are other validated tools (e.g., AUB-HAS2) used in specific contexts. Use the tool whose output will actually change a management step.
Any quick one-liner I can use in the chart?
Try: “RCRI X/6 (Class Y) → est. risk ~Z%; functional capacity ≈N METs; active cardiac conditions absent/present; testing not indicated/ordered as results would/would not alter management; optimization steps completed; proceed with [monitoring plan].” Reddit clinicians repeatedly recommend this level of clarity.
Why do some residents call pre-op “cardiac clearance” voodoo?
Because the value isn’t in a checkbox; it’s in a concise, actionable assessment that sets expectations and plan. Calculators can be misused or ignored if they’re not integrated into decisions. Focus your note on what the team needs to do differently.
Does RCRI cover non-cardiac complications?
No. It’s confined to major cardiac events. Use ACS NSQIP for other outcomes.
Is a “Score ≥3” automatically a hard stop?
No. It signals high risk (≥11%), but the call depends on urgency, optimization potential, functional capacity, and patient goals per guideline steps.
If you need a rcri calculator that’s fast and defensible, this framework works: confirm the six predictors, calculate RCRI, and interpret the bins honestly. For teams that prefer a digital rcri score calculator, pair it with NSQIP when you need procedure-specific outputs. Whether you search for an rcri risk calculator or just perform a quick rcri calculation on paper, the point is the same use it to structure better decisions, not to replace judgment.
References
- Lee TH, et al. Derivation and validation of the Revised Cardiac Risk Index (NEJM 1999). Predictors and creatinine cutoff > 2.0 mg/dL; foundation for the 0–6 score.
- MDCalc: RCRI calculator and commonly cited event rates (0.4%, 0.9%, 6.6%, ≥11%).
- 2024 AHA/ACC Perioperative Guideline: stepwise assessment; use of validated tools like RCRI/NSQIP.
- StatPearls: RCRI overview and predictors; role of functional capacity.
- ACS NSQIP Risk Calculator (for broader outcomes and procedure-specific estimates).
- Comparative performance literature and subgroup caveats.