If you came here for a QTc calculator, you want two things: speed and correctness. Here’s the blunt truth: Bazett’s formula is everywhere, but it misbehaves at high and low heart rates. Fridericia and Framingham typically perform better and should be your defaults. Below is a clean, practical playbook to ensure your qtc calc is clinically defensible without fluff.
QTc Calculator
| Formula | QTc (ms) |
|---|---|
| — | |
Educational tool only. Not a substitute for medical advice.
Explore more heart calculator:
What is QTc (and why you should care)?
QTc is the heart-rate–corrected QT interval. It allows comparison of QT across different heart rates by removing (as best as math can) the effect of RR. Accurate qtc calculation matters because prolonged QTc raises the risk of ventricular arrhythmias, including torsades de pointes. That’s not theoretical risk goes up as QTc climbs.
Measurement basics (don’t skip this):
- Measure QT (ms) from QRS onset to T-wave end in the lead with the longest QT (commonly II, V5, or V6).
- Use the tangent or threshold method for the T-wave end; manual measurement remains the gold standard, especially when the tracing is messy.
- Exclude small, distinct U waves; include large fused U waves.
The formulas your QTc calculator should support
RR is in seconds (RR = 60 / HR). Your qtc formula calculator should output at least these four:
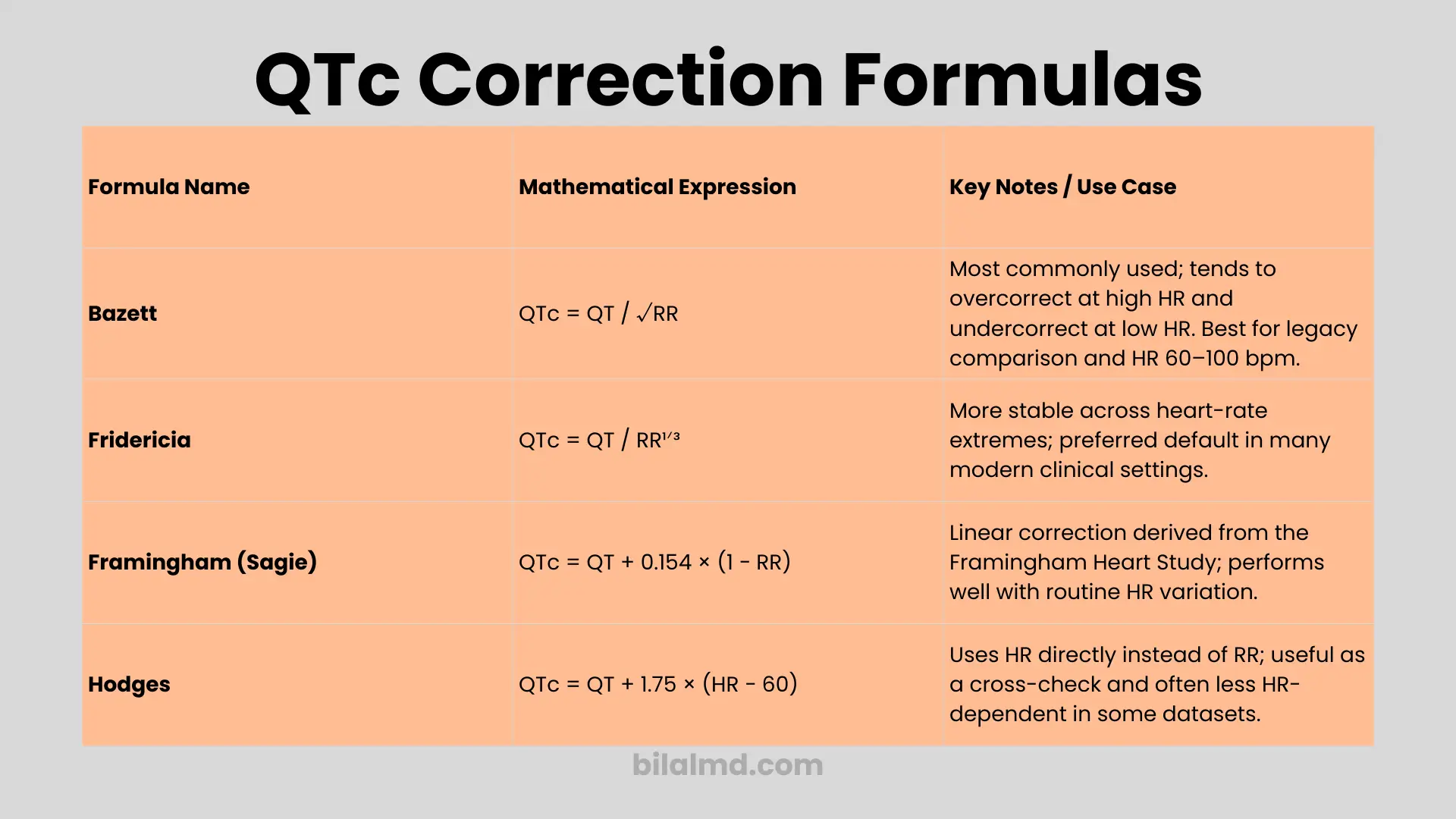
- Bazett’s formula (1920):
QTcB = QT / √RR
Most familiar, but overcorrects at high HR and undercorrects at low HR. Use for legacy comparison or HR 60–100 bpm, but expect bias at extremes. - Fridericia:
QTcF = QT / RR^(1/3)
A stronger default when HR is fast or slow; more stable than Bazett across HR ranges. If you need one primary calculator setting, start here. - Framingham (Sagie):
QTcFram = QT + 0.154 × (1 − RR)
Derived from >5,000 subjects in the Framingham study; widely considered robust across day-to-day HR variation. - Hodges:
QTcH = QT + 1.75 × (HR − 60)
Linear correction; tends to give a narrower QTc spread versus HR in some analyses. Useful as a check.
Evidence snapshot: Multiple comparisons show Bazett performs worst at HR extremes; Fridericia and Framingham generally outperform; Hodges can be least HR-dependent in some datasets. Translation: qtc calculator bazett is fine for quick checks, but Fridericia/Framingham should be your default outputs.
Normal QTc ranges (what “qtc calculation normal range” really means)
- Typical cutoffs used in practice: >440 ms (men) and >460 ms (women) suggest prolonged QTc.
- ≥500 ms is the danger zone and correlates with higher torsades risk; act on it.
- Short QTc (<350 ms) is uncommon and has a different workup.
No sugarcoating: a corrected qt interval calculator is just math. Interpretation and clinical action are on you.
How to calculate QTc step-by-step (use this every time)
- Measure QT across 3–5 beats; choose the longest lead (often II or V5/V6).
- Measure RR in seconds (RR = 60/HR).
- Pick formulas: always compute Fridericia and Framingham; show Bazett and Hodges for reference.
- Document HR and QRS width; if QRS ≥120 ms, see the wide-QRS section.
- Compare your calculated QTc against normal thresholds, and make a decision.
Yes, that answers “how do you calculate qtc,” “how to calculate the qtc,” and “calculating qtc” without hand-waving.
Special case: wide QRS (BBB or pacing) don’t just plug into a standard formula
Big mistake: applying Bazett/Fridericia directly to a BBB/paced ECG. Wide QRS artificially lengthens QT. A pragmatic, evidence-backed strategy is the Bogossian modified QT:
- Modified QT (QTm) = Measured QT − ~50% × QRS
- Then apply your preferred HR correction (Fridericia/Hodges/Framingham) to QTm.
This “subtract 50% of QRS” approach is supported in LBBB and other wide-QRS settings, though variants (e.g., 48.5%) exist in the literature.
Reality check: you’re estimating the “true repolarization” time; different datasets suggest slightly different percentages. Your corrected qtc calculator should prompt for QRS and offer a BBB mode that computes QTm automatically before HR correction.
Which QTc formula should be your primary calculator default?
- Default outputs: Fridericia + Framingham (front and center).
- Also show: Bazett (for legacy comparisons) and Hodges (as a cross-check).
- Warnings: Flag when HR <60 or >100 that Bazett may mislead (over- or under-correction).
- Wide QRS: Ask for QRS; apply Bogossian adjustment before correction.
This layout gives users an honest qtc calc and prevents garbage qtc calculated results at HR extremes or with conduction delay.
Worked examples
Example A: Sinus tachycardia
- HR = 120 bpm ⇒ RR = 0.50 s; measured QT = 320 ms
- Bazett: 320 / √0.50 ≈ 452 ms (inflated; classic over-correction)
- Fridericia: 320 / 0.50^(1/3) ≈ 404 ms
- Framingham: 320 + 0.154 × (1 − 0.50) ≈ 397 ms
Takeaway: At high HR, Fridericia/Framingham better reflect physiology; Bazett exaggerates.
Example B: LBBB (wide QRS)
- HR = 70 bpm ⇒ RR ≈ 0.86 s; QT = 480 ms; QRS = 160 ms
- QTm = 480 − 0.5×160 = 400 ms
- Fridericia QTc = 400 / 0.86^(1/3) ≈ 428 ms
If you had ignored QRS and naively corrected 480 ms, you’d over-call QT prolongation. BBB mode matters.
Practical pitfalls (where most errors happen)
- Measuring the wrong T-end (include biphasic T, exclude discrete U): get this wrong and every qtc formula fails.
- Using Bazett outside 60–100 bpm and treating it as gospel: don’t.
- Ignoring QRS width in BBB/pacing: always adjust first.
- Trusting the machine blindly: auto QTc is a starting point; verify manually when the baseline is messy or waves are fused.
Drug effects: where to check
If your corrected QT calculator screams “prolonged,” confirm meds and interactions against a continuously updated, curated list. CredibleMeds remains the standard public reference for QT-prolonging drugs (risk categories; TdP association). Bookmark it.
FAQs
What is the best QTc calculator formula?
No single winner in all contexts, but Fridericia and Framingham usually beat Bazett at HR extremes; Hodges can be least correlated with HR in some sets. That’s why a multi-output qtc calculator formula is the practical approach.
What is the “qtc calculation normal range”?
Commonly used thresholds: >440 ms (men) or >460 ms (women) are prolonged; ≥500 ms implies higher torsades risk and demands attention.
How to calculate QTc (aka “how do you calculate qtc / how to calculate the qtc / calcul qtc”)?
Measure QT and RR, then apply Fridericia/Framingham (always display Bazett/Hodges). Document QRS and use BBB mode if QRS ≥120 ms.
Should I use a fridericia qtc calculator over Bazett’s formula?
If HR is <60 or >100, yes Fridericia or Framingham will typically be more reliable. Keep Bazett’s formula for legacy comparison.
Does a corrected qt interval calculator work in bundle branch block?
Only after you compute QTm (e.g., QT − ~50% × QRS) and then correct QTm for HR. Otherwise you’ll over-estimate repolarization time.
Can I trust the ECG machine’s qtc calculated number?
Treat machine output as screening. For curved baselines, fused T-U, or noisy signals, manual measurement using the tangent/threshold method is preferred by expert guidance.
Is QTc 480 ms dangerous?
Borderline-high; context rules. Persistent ≥500 ms is the clearest red flag. Review meds/electrolytes and clinical status; consider cardiology input.
Why does my patient’s QTc jump when HR changes?
Because the correction is imperfect. Different formulas behave differently as HR drifts. Fridericia/Framingham tend to be less HR-dependent than Bazett.
Final word
A qtc calculator is a tool, not a verdict. If your qtc calculated value is ≥500 ms or if there are concerning symptoms, interacting meds, or electrolytes out of range escalate. For your primary calculator defaults, show Fridericia and Framingham, keep Bazett visible (with warnings), and always handle wide QRS via a modified QT before correction. That’s how you stop making the common mistakes and start making better decisions.
Disclaimer: This page is for educational use and tool guidance only; it is not a substitute for clinical judgment or specialist consultation.
References
- Manual vs auto QTc; tangent/threshold method; measure in II/V5; exclude discrete U.
- Formulas and their behavior (Bazett, Fridericia, Framingham, Hodges); RR in seconds.
- Why Bazett is unreliable at extremes; Fridericia/Framingham preferred; mortality prediction data.
- Comparative studies showing Bazett underperforms; Hodges least HR-dependent in some sets.
- Wide-QRS/BBB approach (Bogossian modified QT; ~50% of QRS); variations like 48.5%.
- CredibleMeds (drug lists & background explainer PDF).