If you work in emergency care you have probably heard of the PERC calculator. It is a fast bedside way to decide if a patient with possible pulmonary embolism can safely avoid further testing. Used correctly it saves time, reduces unnecessary imaging, and spares patients anxiety and radiation. Used incorrectly it can mislead. This guide explains the PERC calculator in clear language, shows exactly when and how to use it, and highlights the pitfalls you must avoid.
PERC Calculator – Pulmonary Embolism Rule out Criteria
Use only when the patient has a low pretest probability of pulmonary embolism by clinical judgment or a low formal risk score. If all eight criteria are met the patient is PERC negative and further testing is usually unnecessary. All 8 met = PERC negative
Definitions and tips
- Low pretest probability: clinician gestalt around fifteen percent or less, or low by Wells or revised Geneva.
- Recent surgery or trauma: within four weeks requiring treatment or immobilization.
- Estrogen use: combined hormonal contraception or estrogen replacement therapy.
- Oxygen saturation: measure on room air. Consider altitude adjusted thresholds in high altitude practice.
Disclaimer
This calculator is for education and clinical decision support. It does not replace clinician judgment, local policy, or specialist consultation. If the patient is not clearly low risk do not use the PERC rule to exclude pulmonary embolism.
Explore more heart calculator:
What the PERC calculator actually is
PERC stands for Pulmonary Embolism Rule out Criteria. It is a set of eight yes or no items designed to rule out pulmonary embolism in adults who already appear low risk based on clinical judgment. Large professional guidelines endorse this approach for low risk patients because it safely reduces needless testing.
The rule was derived and tested in emergency departments and is now widely used. The original research defined the eight items and demonstrated that in carefully selected low risk patients the rule can exclude pulmonary embolism without further tests.
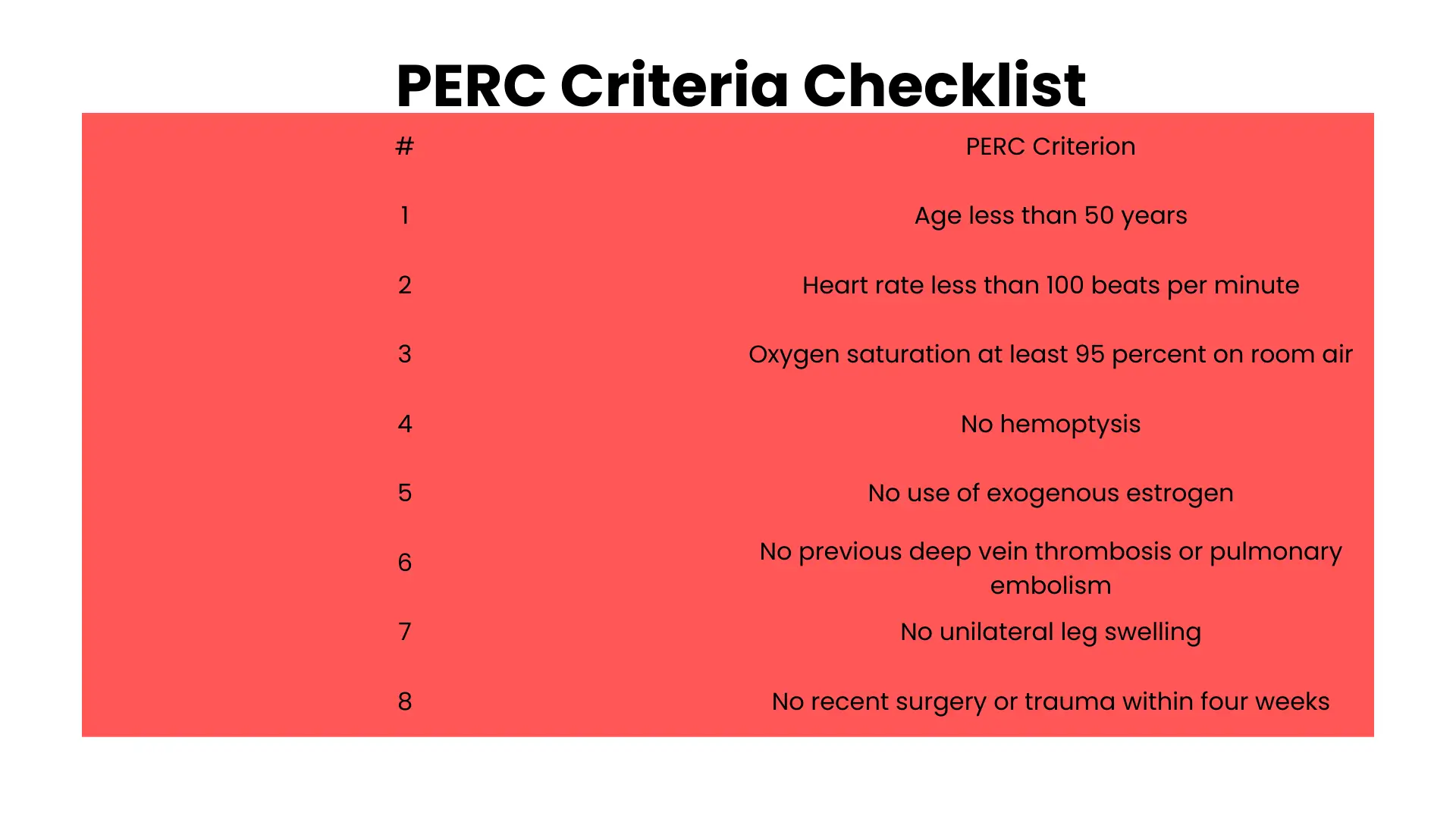
The eight PERC items in plain words
To consider a patient PERC negative every single statement below must be true. If even one is not true then the patient is PERC positive and you should continue the workup.
- Age is less than fifty years
- Heart rate is under one hundred beats per minute
- Oxygen saturation on room air is at least ninety five percent
- There is no unilateral leg swelling
- There is no coughing of blood
- There has been no recent surgery or significant trauma that required hospital care within the last four weeks
- There is no previous history of deep vein thrombosis or pulmonary embolism
- There is no current use of exogenous estrogen
Most clinical calculator sites present the thresholds as written above, while the original derivation used a very similar oxygen saturation threshold and otherwise the same clinical statements.
The one rule you must remember before you ever click Calculate
Only apply the PERC calculator to patients who are truly low risk. That means your pretest probability by gestalt or by a low Wells or Geneva assessment is about fifteen percent or less. In those patients a completely negative PERC result allows you to stop without a D dimer or imaging. This is exactly how the rule was studied and how major emergency medicine policies advise using it.
Step by step use at the bedside
- Start with clinical judgment. If your overall suspicion is not low then stop. PERC is not for this patient.
- If the patient seems low risk, run through the eight items quickly and carefully.
- If all eight statements are true the patient is PERC negative and you can go further tests in most settings.
- If any item is not true the patient is PERC positive. Proceed with standard testing such as D dimer or imaging as appropriate to your pathway.
This workflow aligns with the prospective studies and with widely used reference implementations.
How well the PERC calculator performs
In a large prospective multicenter study combining a clinician’s low suspicion with a negative PERC result safely reduced unnecessary testing in emergency departments. Later meta analyses and reviews reported very high sensitivity and a low negative likelihood ratio, consistent with a very small miss rate when used in the correct population.
Policy writers use those data to recommend PERC as a safe strategy for low risk adults. Keep in mind that these numbers assume careful patient selection and strict application of all eight items.
Where the PERC calculator can fail
No decision tool is perfect. Several groups have warned about misuse of PERC in populations that were not well represented in the original work or in settings with a higher baseline prevalence of pulmonary embolism.
Pregnancy and the early postpartum period are special situations. Evidence is limited and expert summaries caution against using PERC by itself in these patients. Other structured pathways exist for pregnancy that combine clinical assessment with tailored testing.
Children and teenagers require caution. Pediatric studies to date are small or retrospective and emphasize the need for dedicated validation before routine use.
Some European cohorts with higher disease prevalence have reported lower performance, which reinforces the need to understand your local prevalence before you lean on any rule to dismiss disease.
Special topic: oxygen saturation cutoffs and altitude
Most bedside tools treat oxygen saturation below ninety five percent on room air as a positive PERC item. The original derivation used a value very close to that threshold. At high altitude an altitude adjusted version of the rule increases the allowance for lower saturation. Clinicians practicing above about four thousand feet can consider altitude adjusted thresholds as presented in decision support calculators.
PERC calculator compared with Wells and Geneva scores
Think of PERC as a gatekeeper that lets you stop when risk is already very low. It is not meant to prove disease and it is not a replacement for broader risk estimates. Wells and revised Geneva assign points and sort patients into probability bands. PERC is different. It gives you permission to stop when your pretest probability is already low and all eight items are satisfied. Teaching resources and clinical sites consistently frame the tools this way and guidelines explicitly support PERC for low risk adults.
A quick example to make it concrete
A middle aged woman arrives with pleuritic chest pain after a long car ride. She is anxious but her oxygen saturation is ninety eight on room air. Her pulse is ninety two. She has no leg swelling, no coughing of blood, no recent surgery or trauma, and no history of clots. She is not using estrogen therapy. Your overall impression after exam and review is that risk is low. Because every PERC item is satisfied she is PERC negative. In a guideline based pathway you can stop without ordering a D dimer or imaging. This use mirrors both the studies and the clinical policies.
Practical tips that keep you out of trouble
Speak the items out loud and document each one. It prevents missed details.
Treat any positive item as a stop sign. Move to testing rather than bending the rule.
Do not apply PERC to medium or high risk patients. That is outside the evidence.
Remember that chronic leg edema and long standing anemia can confuse the exam. When in doubt escalate to testing.
For high altitude practice review the altitude adjusted approach before your next shift.
Frequently asked questions about the PERC calculator
Do I need a D dimer if my patient is PERC negative and truly low risk
No. That is precisely the point of the rule and why policies endorse it. If every item is satisfied in an adult who is already low risk you can stop without further testing.
Can I use the PERC calculator in pregnancy
Not as a stand alone rule. Pregnancy and the early postpartum window were not well validated for PERC and expert sources advise alternative structured pathways for those patients.
Does birth control count as estrogen use for the rule
Yes. The estrogen item is considered positive when a patient is taking exogenous estrogen. Combination hormonal contraception is a common reason this item becomes positive.
My patient is on a beta blocker and the pulse is in the nineties. Can I trust that heart rate item
Be careful. The rule assumes a true physiologic pulse under one hundred, not a medication masked value. Many educators caution against relying on a medicated heart rate when overall suspicion is not clearly low. If you are uneasy, do not use PERC to stop the workup.
What about children or teenagers
Routine use is not recommended. Early studies are small and emphasize the need for more validation. Use age appropriate pathways and clinical judgment.
Can I use PERC in a region with a high baseline prevalence of pulmonary embolism
Use caution. Studies from higher prevalence settings have shown weaker performance. In such environments many teams prefer a D dimer first strategy even when the patient seems low risk.
Is there a version for high altitude practice
Yes. An altitude adjusted PERC tool exists and raises the acceptable oxygen saturation threshold for clinicians working well above sea level. Check the calculator details before use.
What sensitivity should I expect if I use the rule correctly
Syntheses of multiple studies report very high sensitivity when PERC is applied to low risk adults, with a small accepted miss rate. Your real world numbers depend on population and adherence to the rule.
Bottom line
The PERC calculator is powerful precisely because it is simple. Choose the right patient first. Then check all eight items with care. If every item is satisfied you can stop without more tests in most low risk adults. Follow your local policy, know the exceptions, and do not let convenience overrule judgment. When you use the PERC calculator the way it was intended you protect patients from unnecessary tests while keeping safety front and center.