Use the Padua Scoring calculator above to total the Padua Prediction Score in real time. Select the risk factors, confirm the total, and use the interpretation guide below to decide on prophylaxis for venous thromboembolism in adult medical inpatients.
Padua Score Calculator
Select all risk factors present at admission, then calculate the Padua score.
Explore more heart calculator:
Pauda scoring guide for medical inpatients
Pauda scoring, also called the Padua Prediction Score, is a practical way to estimate the risk of venous thromboembolism in hospitalized medical patients. The method was derived in a large study of acutely ill adults and has been validated in multiple settings. The rule is simple. Add the points for each present risk factor. A total of four or more indicates a high risk of venous thromboembolism. A total below four indicates low risk. The score serves as a starting point for making a clinical decision about pharmacologic prophylaxis, taking into account the bleeding risk and procedural plans.
What pauda scoring measures and why it matters
Hospitalization amplifies the classic drivers of clot formation. Immobility promotes venous stasis. Acute illness and procedures can increase inflammation and activate the coagulation process. Some patients also carry baseline risks such as cancer or inherited thrombophilia. Pauda scoring counts the most predictive clinical features and converts them into a total that stratifies risk with a clear threshold. In the original study, patients with a total of four or more had a much higher event rate when not given prophylaxis, while those below four had a very low event rate. This separation helps clinicians focus medication on those who benefit most and avoid unnecessary exposure in the low-risk group.
The exact Padua items and points
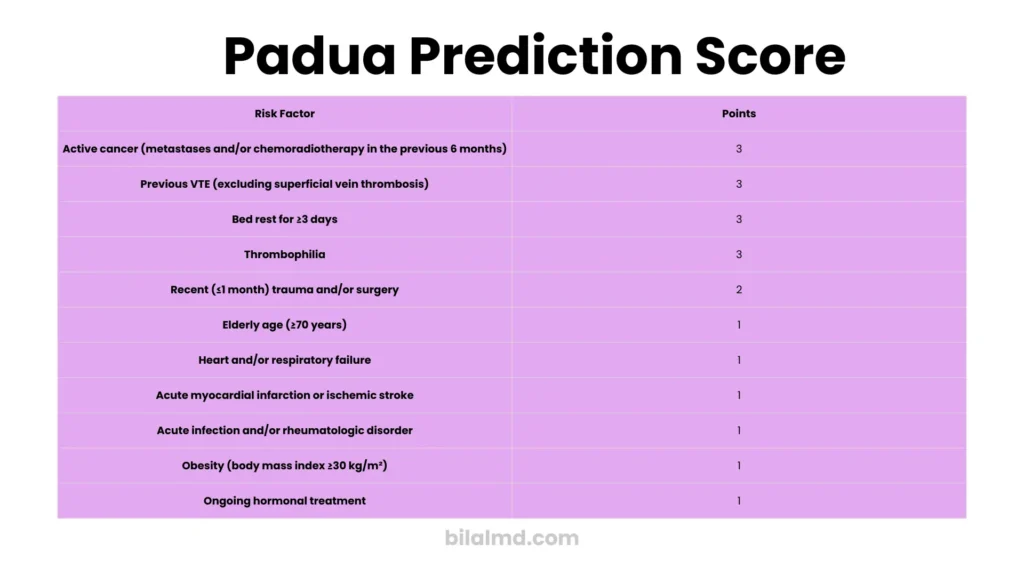
The calculator on this page uses the standard items from the original model.
Three points each
- Active cancer, including treatment within six months or palliative care
- Previous venous thromboembolism, excluding isolated superficial thrombophlebitis
- Reduced mobility is defined as expected bed rest with bathroom privileges for at least three days
- Known thrombophilia such as factor V Leiden, prothrombin G20210A, protein C or protein S deficiency, antithrombin deficiency, or antiphospholipid syndrome
Two points
- Recent trauma or surgery within one month
One point each
- Age of at least seventy years
- Heart failure or respiratory failure
- Acute myocardial infarction or ischemic stroke
- Acute infection or rheumatologic disorder
- Body mass index of thirty or more
- Ongoing hormonal treatment, such as estrogen therapy or selective estrogen receptor modulators
The threshold for high risk is a total of four or more.
How to use the result from the calculator
- Confirm the total. Four or more is high risk. Less than four is low risk.
- Screen for bleeding risk before ordering a drug. Consider platelet count, active bleeding, recent major bleeding, planned neuraxial procedures, and severe coagulopathy.
- Choose a prophylaxis path.
- High risk with acceptable bleeding risk: pharmacologic prophylaxis is usually appropriate.
- High risk with unacceptable bleeding risk: use mechanical methods and reassess daily.
- Low risk: prioritize early mobilization and consider mechanical methods based on protocol.
These steps reflect widely used guidance from hematology societies for adult medical inpatients.
What to give when the patient is at high risk
Common choices for pharmacologic prophylaxis in medical inpatients are low molecular weight heparin once daily in typical weight ranges or low-dose unfractionated heparin given two or three times daily. Preference for low molecular weight heparin in this population is supported by hematology guidelines, with attention to renal function and weight-based adjustments according to local protocol. If renal function is markedly reduced or rapid reversal is a priority, unfractionated heparin may be preferred.
Mechanical options include intermittent pneumatic compression for patients who cannot receive pharmacologic prophylaxis or as an adjunct in very high-risk cases. Ensure correct sizing and adherence, since poor fit reduces effectiveness.
Practical bedside examples
- Elderly patient with pneumonia and poor mobility
Age at least seventy equals one point, respiratory failure equals one point, and reduced mobility equals three points. Total equals five, which is high risk. If there is no major bleeding concern, pharmacologic prophylaxis is reasonable. - Patient with active cancer on chemotherapy who is in bed
Active cancer equals three points. Infection during neutropenia equals one point. Reduced mobility equals three points. Total equals seven, which is high risk. Start pharmacologic prophylaxis if there is no contraindication. - Middle-aged patient with cellulitis who is walking to the chair and bathroom
Obesity at one point, without other factors, often remains below four. Low risk supports a plan centered on early ambulation and monitoring.
When pauda scoring is not enough by itself
The score estimates the probability of venous thromboembolism but does not tell you whether the patient is safe to anticoagulate. Always apply a bleeding risk lens and a procedural plan. Major society guidance stresses this two-step approach. For example, the American Society of Hematology recommends low molecular weight heparin over direct oral agents for acutely ill medical inpatients who require prophylaxis, and it provides separate advice on which populations should not receive routine pharmacologic prophylaxis. Use your hospital pathway if available and document your reasoning.
Documentation that stands up to audit
Good documentation is fast and protective.
- Record the total pauda scoring result and list the selected factors.
- State whether the bleeding risk is acceptable and if any procedure is planned.
- Write the chosen agent and dose or the reason for using mechanical methods only.
- Reassess and update if mobility improves or clinical status changes.
A single-line template you can paste into a note
Padua total of five based on reduced mobility, age of at least seventy, and respiratory failure. No bleeding contraindication. Start low molecular weight heparin per protocol. Reassess tomorrow.
Strengths and limitations of pauda scoring
Strengths
- Transparent criteria that match common clinical information at admission
- A clear threshold of four that separates high and low risk groups
- Independent validation in different cohorts and easy integration into admission workflows
Limitations
- The score does not account for every nuance, such as planned neuraxial anesthesia or severe thrombocytopenia, which are contraindications to drugs.
- Some items are broad, such as infection or reduced mobility, and need consistent local definitions.
- Other models exist, such as IMPROVE, which can be paired with an explicit bleeding score in some pathways; hospitals may favor one model based on local performance and workflow.
Frequently asked questions
If the total is four do I always need to start a drug
No. Four or more signals are high risk for clotting. You still need to confirm that the bleeding risk is acceptable and that no procedure will conflict with anticoagulation. Use mechanical methods if medication is unsafe today and reassess tomorrow. This aligns with hematology guidance.
What exactly counts as reduced mobility
Use the definition from the model. Bed rest with bathroom privileges is expected for at least three days. A patient who walks several times daily to the chair and hallway usually does not meet this item.
Should I add prophylaxis if the patient is already on full dose anticoagulation for another reason?
No. Therapeutic anticoagulation covers prophylaxis. Do not add more. This is consistent with expert guidance and common practice standards.
What about patients on antiplatelet therapy
Antiplatelet drugs reduce arterial events and do not replace anticoagulant prophylaxis for venous events. Use the score and bleeding risk assessment to decide.
Which agent is preferred for acutely ill medical inpatients
Many pathways prefer low molecular weight heparin over direct oral agents during the inpatient phase. Choice always depends on renal function, weight, procedural timing, and local formulary.
How often should I rescore
At least daily for unstable patients, and whenever mobility or procedural plans change. The original derivation and validation emphasize dynamic reassessment in response to clinical change.
Pauda scoring versus alternative tools.
Some hospitals use IMPROVE for VTE risk and a separate IMPROVE bleeding score to balance decisions. Evidence continues to evolve, and some analyses compare the discrimination and calibration of different tools across settings. The key is a consistent local standard and clear documentation of why a patient did or did not receive pharmacologic prophylaxis.
Step-by-step workflow to use with the calculator
- Select all applicable Padua risk factors at admission.
- Confirm the total and note the risk category.
- Screen for bleeding risk and any procedures.
- If high risk and safe, start pharmacologic prophylaxis and add early mobilization.
- If not safe for medication, use mechanical methods and reassess.
- Recheck the score and plan each day as mobility or diagnoses change.
References and further reading
- Contemporary public health sheet summarizing Padua criteria and threshold for high risk. Queensland Health 2025.
- Barbar S, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism. Original Padua Prediction Score derivation. J Thromb Haemost. 2010.
- External validation and summary of Padua and IMPROVE risk models, including item list and high-risk threshold. 2023.
- ASH clinical practice guideline on prophylaxis for medical patients. Snapshot and full guideline. 2018.
- Event rates by Padua category and practical calculator summary. Medscape Calculator.
- Reviews of VTE prophylaxis in medically ill patients, including recommended inpatient agents and when not to use routine pharmacologic prophylaxis.
- Comparative performance of medical inpatient VTE risk assessment models, including IMPROVE and Geneva families. JAMA Network Open 2024.
- Recent work on IMPROVE decision strategies that combine VTE and bleeding risk in modern cohorts. Blood Advances 2024.