A HEART Score Calculator helps clinicians quickly estimate the short term risk of major adverse cardiac events after a patient arrives with chest pain. It is simple, fast, and practical, which is why emergency departments all over the world use it as part of structured decision making. The goal is not to replace clinical judgment. The goal is to make a clearer and safer decision about observation, testing, or discharge based on consistent criteria supported by evidence.
Explore more heart calculator:
What the HEART score measures
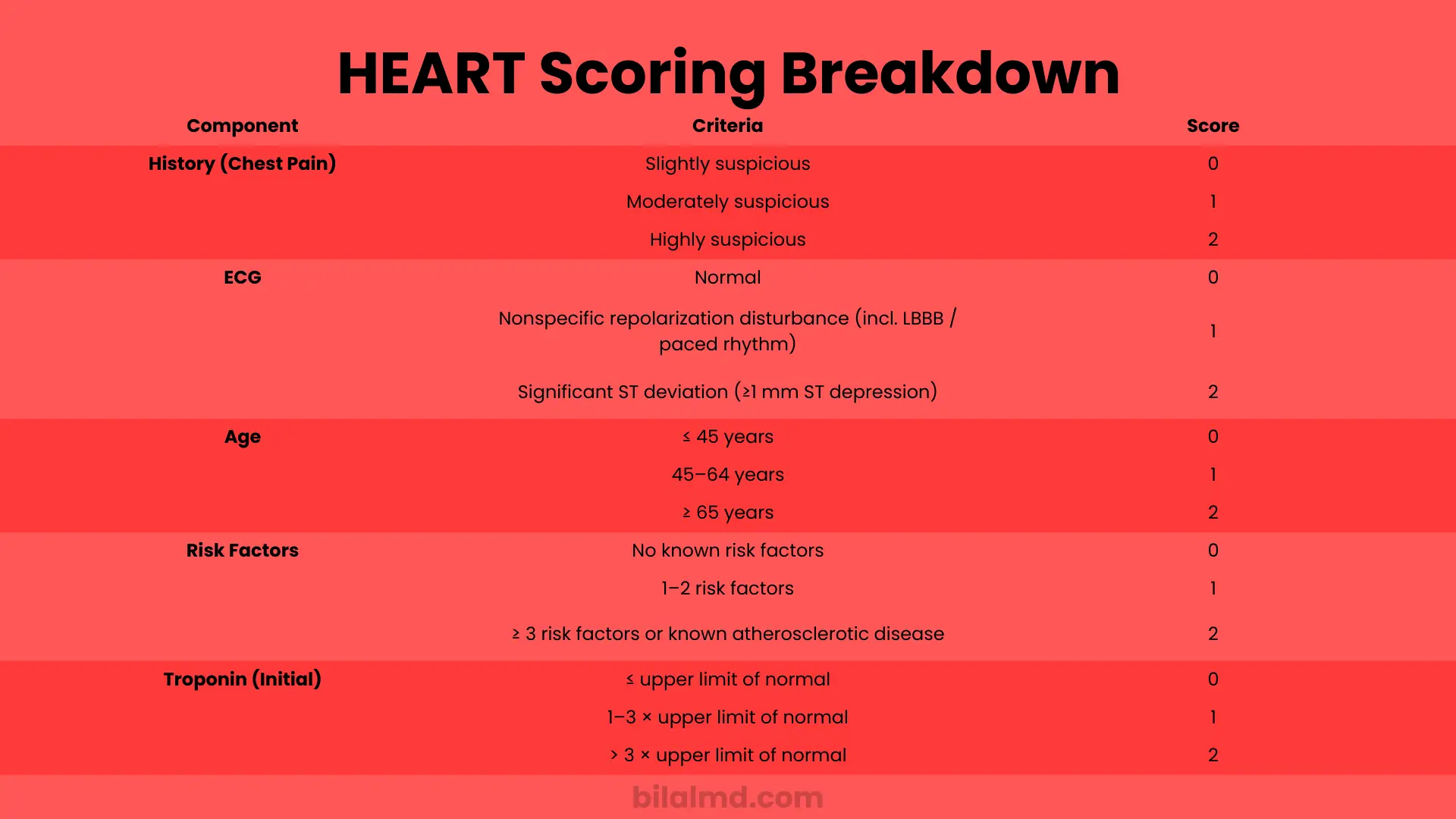
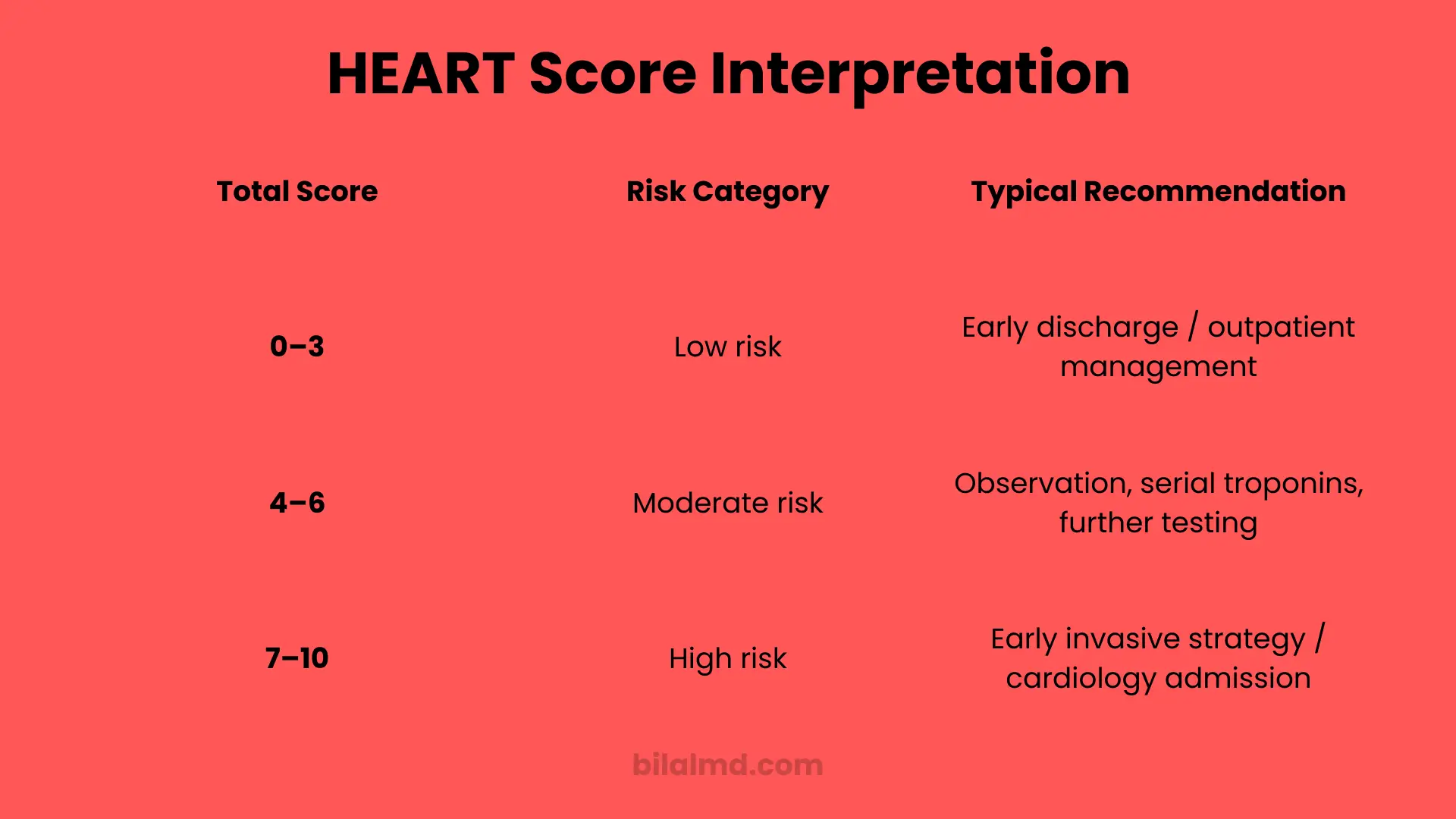
HEART is an acronym for History, ECG, Age, Risk factors, and Troponin. Each element receives a value of zero, one, or two. The total ranges from zero to ten. Scores of zero to three typically indicate low short term risk, four to six indicate moderate risk, and seven to ten indicate high risk. The score uses information you already collect at the bedside, so it adds almost no friction to normal care.
Why the HEART Score Calculator matters
The score did not become popular because of a catchy name. It became popular because it predicts outcomes with solid performance and clear cutoffs. In a large prospective validation, patients with a total of zero to three had about one to two percent risk of a major adverse cardiac event in the next weeks. Those with four to six had about seventeen percent risk, and those with seven to ten had about fifty percent risk. These bands help teams decide who can go home with follow up and who needs further testing or admission. The same study showed stronger discrimination than TIMI and GRACE in the emergency setting.
The five parts of the score
History
This is the overall clinical impression of how typical the chest pain seems for an ischemic cause. Slightly suspicious patterns score lower than very typical patterns with classic features. Clinical judgment still matters here.
ECG
A normal tracing scores lower. Nonspecific repolarization changes score in the middle. Clear ischemic changes such as at least one millimeter of ST depression score higher.
Age
Younger age lowers the total. Middle age increases it slightly. Older age increases it more, reflecting baseline risk.
Risk factors
Common cardiovascular risk factors raise the total. These include hypertension, diabetes, high cholesterol, smoking, obesity, and family history. Established atherosclerotic disease such as prior coronary or peripheral arterial disease also increases the score.
Troponin
A normal troponin at presentation scores lowest. Rising levels relative to your laboratory upper reference limit raise the score. Today many hospitals use high sensitivity cardiac troponin assays, which detect smaller changes earlier. The principle is the same, but the pathway often adds serial measurements to improve safety.
Interpreting the total
- Low risk total of zero to three
Short term risk is around one to two percent in the classic validation. Many sites consider early discharge with timely follow up when the clinical picture, ECG, and serial troponins are reassuring. - Moderate risk total of four to six
Risk is meaningfully higher. These patients usually need observation, serial troponins, and often noninvasive testing depending on local protocols and clinical judgment. - High risk total of seven to ten
Risk is high enough that urgent inpatient evaluation is common. These patients frequently proceed to advanced testing or intervention based on evolving data.
HEART Score versus HEART Pathway
The raw score is just a number. The HEART Pathway turns that number into a structured decision aid by pairing it with timed troponin testing, usually at zero and three hours. In a randomized trial, the pathway increased the rate of safe early discharge, reduced unnecessary testing, and did not increase missed events at thirty days. The pathway has since been replicated and extended, including with high sensitivity assays.
How high sensitivity troponin fits in
Modern guidelines recommend high sensitivity troponin as the preferred biomarker for myocardial injury. Many hospitals now run accelerated diagnostic protocols that combine the HEART framework with serial high sensitivity troponin using assay specific cutoffs. Implementations have shown more discharges, fewer admissions, and no increase in short term adverse outcomes when applied properly.
When you should not lean on the score
A calculator helps only when the setting fits. The score was built for undifferentiated chest pain in adults without clear ST elevation and without obvious alternative diagnoses. It does not replace judgment in patients with unstable vital signs, ongoing severe ischemic symptoms, dynamic ischemic changes, or clear noncardiac causes that still require urgent care such as aortic pathology or pulmonary embolism. Use guideline based pathways to rule in or rule out myocardial infarction and then use the score to support disposition if the picture remains uncertain.
A simple step by step way to use a HEART Score Calculator
- Gather the basics
Record the history, the ECG reading, the age, the risk factors, and the initial troponin result. Try to keep the history judgment consistent across your team by using agreed prompts. - Assign the values
For each of the five parts choose zero, one, or two. Consistency matters more than perfection because the score performs as a bundle. - Add it up
Sum the five values to get a total from zero to ten. - Place the patient in a band
Use low, moderate, or high bands to frame the next decision. Do not stop here. - Layer in troponin timing
If you use the HEART Pathway, repeat troponin at about three hours and reassess. A stable normal pattern supports early discharge in low totals. - Decide disposition
Low total with reassuring pathway steps usually means discharge with clear return precautions and timely follow up. Moderate totals often stay for observation or testing. High totals stay for urgent inpatient workup.
Example walk through
A fifty four year old presents with pressure like chest discomfort that started while walking and eased with rest. The ECG shows nonspecific changes without clear ischemia. The patient has hypertension and high cholesterol but no prior coronary disease. The first high sensitivity troponin is within the reference range.
- History feels moderately suspicious, so one
- ECG is nonspecific, so one
- Age is forty five to sixty four, so one
- Risk factors are one to two, so one
- Troponin is normal, so zero
The total is four, which is in the moderate band. Following the pathway you repeat troponin at three hours. If both measurements stay within reference and the clinical picture remains stable, you discuss observation with possible noninvasive testing based on shared decision making and local practice.
Strengths and limitations you should know
Strengths
The score is fast, reproducible across clinicians, and validated in large cohorts. It improves consistency and helps right size testing and admission. It integrates well with accelerated diagnostic protocols that use modern biomarker assays.
Limitations
The history component is subjective. The score should not be used in isolation to override obvious red flags. It also does not resolve every edge case such as very early presenters with evolving symptoms or patients with complex comorbid disease that confounds interpretation. Methodologic appraisals have called out variability across studies and urged careful attention to implementation. Use the tool inside a guideline based pathway and always combine it with clinical judgment.
Practical tips for teams
- Build a short script that standardizes how you judge the history
- Document the five parts in the same order every time
- Use your laboratory’s exact upper reference limit when interpreting troponin
- Train nurses and physicians together so the pathway steps are consistent
- Audit discharges with low totals to confirm outcomes and refine local instructions
These simple steps help the calculator deliver consistent safety and efficiency in real practice.
FAQs
Is a low HEART score safe to send a patient home
Evidence shows that patients with totals of zero to three have a very low short term risk when paired with serial troponin and a reassuring ECG. Many programs safely discharge such patients with clear return precautions and timely follow up.
What is the difference between the HEART score and the HEART Pathway
The score is the five part number from zero to ten. The pathway adds timed troponin testing and explicit actions. Trials show the pathway increases safe early discharges and reduces unnecessary testing.
Does the score still work with high sensitivity troponin
Yes. Guidelines prefer high sensitivity assays and many centers have integrated them into HEART based pathways with good safety and efficiency when used correctly.
Is the HEART score better than TIMI in the emergency department
In the prospective validation, the score showed stronger discrimination than TIMI and GRACE for emergency presentations of chest pain. The best approach is to follow a decision pathway that your site has adopted and validated.
Can I use the score if the first troponin is normal
Yes, but do not stop at a single result. The pathway relies on serial measurements to catch early injury. Repeat testing at about three hours is common practice.
What counts as a risk factor inside the score
Hypertension, diabetes, high cholesterol, smoking, obesity, and a family history of early coronary disease are typical. Known atherosclerotic disease also counts.
Does using the score reduce admissions and costs
Pathway research shows more early discharges, fewer admissions, and less downstream testing when the tool is implemented well. That is why many systems have standardized it.
Can young patients with a low score still have a heart attack
Yes. No tool is perfect. A low total reduces risk but does not make it zero. Use repeat troponin, careful discharge instructions, and clinical judgment.
Can the HEART score be used in pregnancy
Use great caution. Physiologic changes and differential diagnoses can complicate interpretation. Follow guideline based evaluation with specialist input.
Bottom line
A HEART Score Calculator is most powerful when it is part of a structured pathway with serial troponin and clear actions. Use it to standardize decisions, not to replace thinking. When you keep the steps tight and the follow up clear, you will protect patients from both under testing and over testing while keeping your emergency department moving safely.
Key sources
Foundational validation of low, moderate, and high risk bands and their approximate event rates.
Practical application guidance for the five part score in emergency care.
Randomized trial and implementation studies of the pathway and its impact on discharges and testing.
Guideline perspective on the preferred use of high sensitivity troponin in chest pain evaluation.