The HAS BLED calculator (a.k.a. HAS-BLED score calculator) is a simple 0–9 risk score that estimates 1-year major bleeding risk in adults with atrial fibrillation (AF). It was derived from the Euro Heart Survey and published in 2010; each letter is one point if present: Hypertension, Abnormal renal, Abnormal liver, Stroke, Bleeding history/predisposition, Labile INR, Elderly (≥65), Drugs predisposing to bleed (antiplatelet/NSAID), Drugs/alcohol (≥8 drinks/week).
HAS-BLED Calculator
Estimates 1-year major bleeding risk in atrial fibrillation. Educational use only.
Total score: 0 / 9
Risk category: Low
—
Medical Disclaimer: This HAS-BLED calculator is for educational and informational purposes only and does not constitute medical advice. Clinical decisions must be made by qualified healthcare professionals using full patient history and current guidelines. HAS-BLED identifies modifiable bleeding risk factors and must not be used alone to withhold anticoagulation therapy.
Explore more heart calculator:
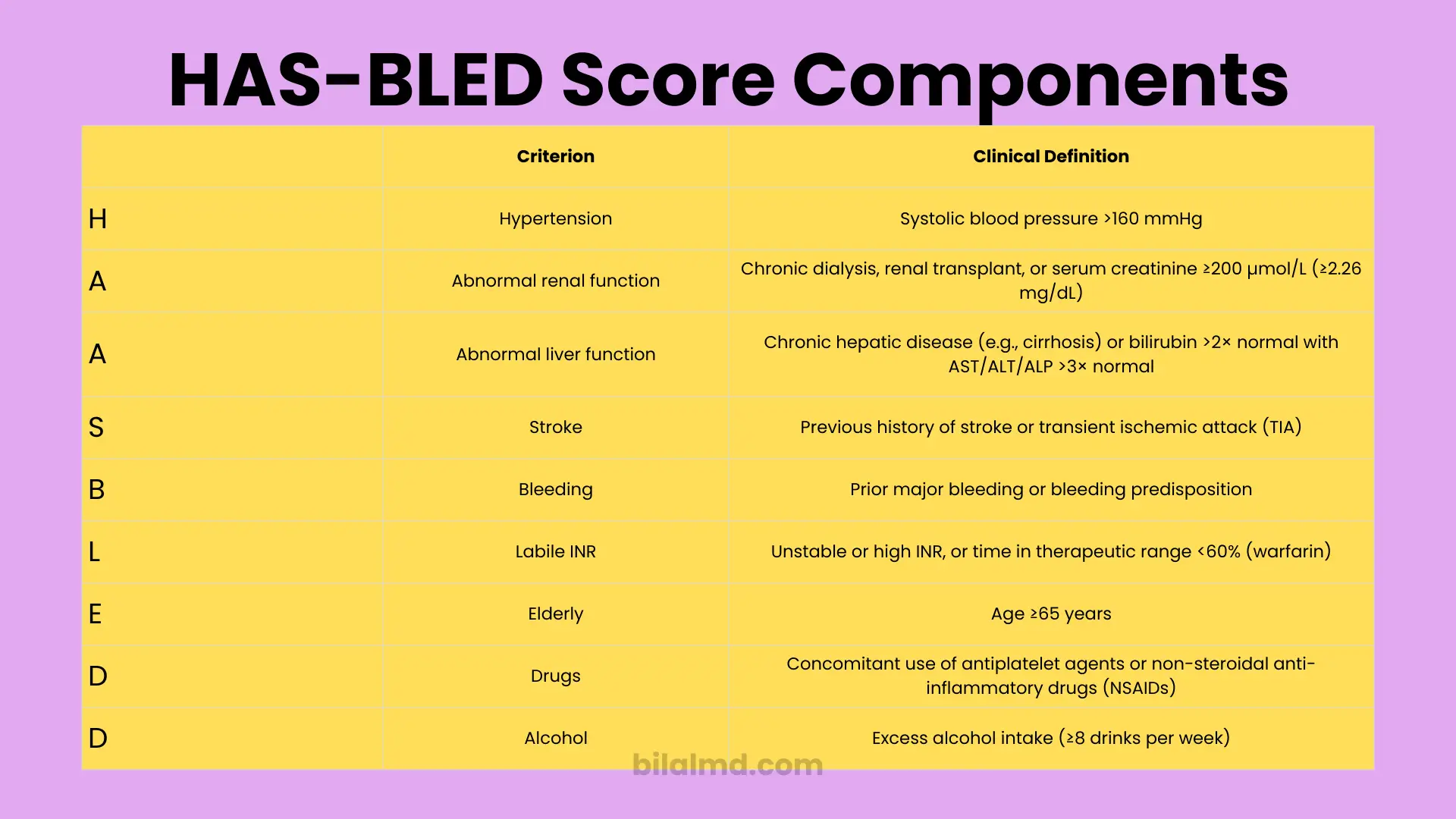
What counts for each letter
- H – Hypertension: Systolic BP >160 mmHg (uncontrolled).
- A – Abnormal renal: Dialysis, transplant, or creatinine ≥200 μmol/L (≈2.26 mg/dL).
- A – Abnormal liver: Chronic liver disease or bilirubin >2× normal with AST/ALT/AP >3× normal.
- S – Stroke/TIA: Prior ischemic stroke/TIA.
- B – Bleeding: Prior major bleed or predisposition (e.g., anemia/bleeding diathesis).
- L – Labile INR: Poor time-in-therapeutic range on warfarin (classically TTR <60–65%).
- E – Elderly: Age ≥65 years.
- D – Drugs: Concomitant antiplatelet agent or NSAID use.
- D – Alcohol: ≥8 drinks/week.
These definitions reflect the original paper and widely used clinical references.
Interpreting your HAS-BLED score
From the original cohort’s observed 1-year major bleeding rates:
- Score 0 ≈ 1.13%
- 1 ≈ 1.02%
- 2 ≈ 1.88%
- 3 ≈ 3.74%
- 4 ≈ 8.70%
- 5 ≈ 12.50%
(Above 5, data were sparse in the derivation cohort.) Use these as ballpark figures; contemporary populations and DOAC-heavy practice patterns can differ.
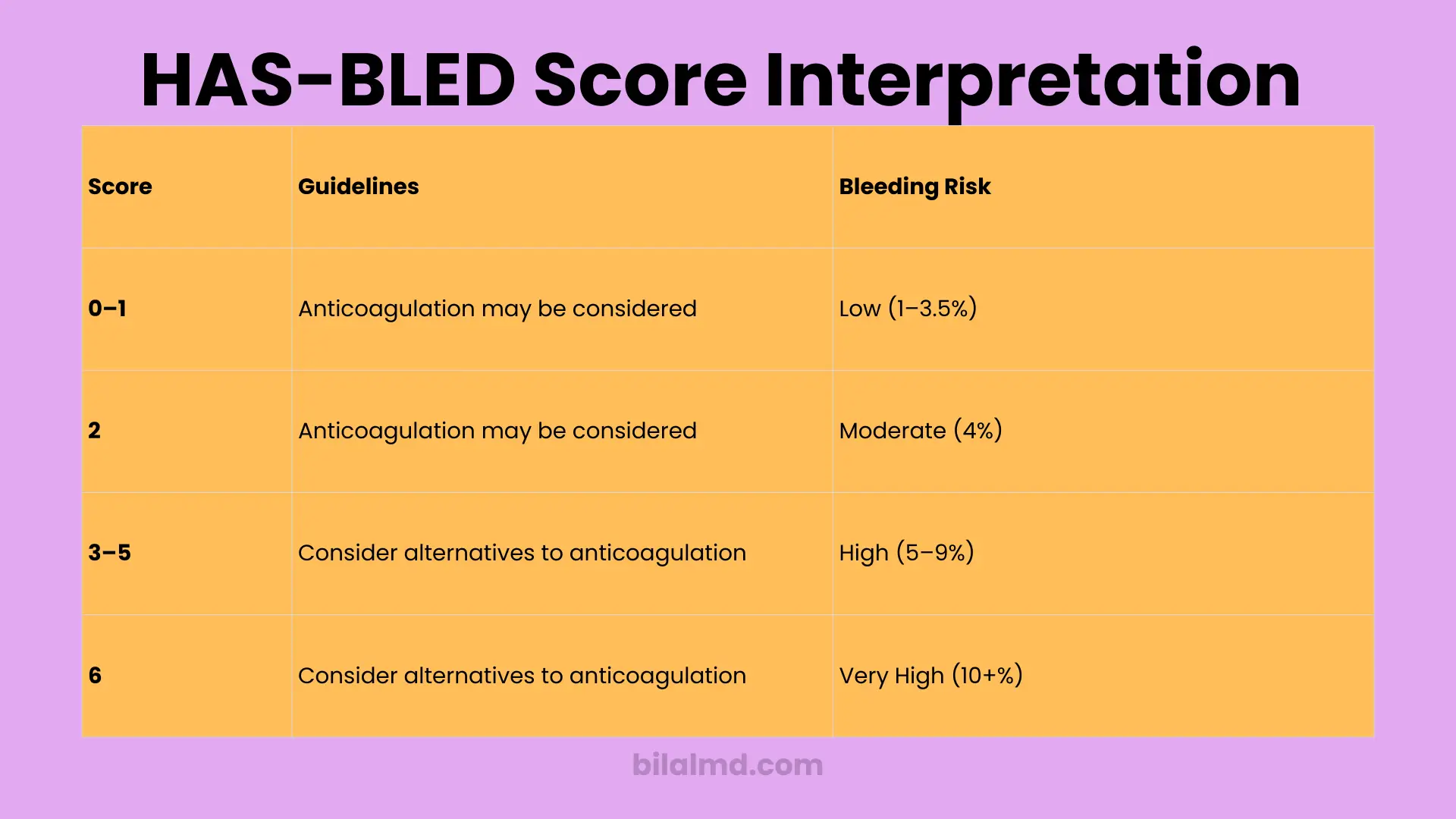
Practical categories used in clinics
- Low: 0
- Moderate: 1–2
- High: ≥3 (warrants closer review/monitoring and aggressive risk-factor management; it does not automatically mean “no anticoagulation”).
What the HAS-BLED calculator is good for
Good for
- Making you look for fixable problems: uncontrolled BP, unnecessary NSAIDs/dual antiplatelets, alcohol excess, poor warfarin control, untreated renal/liver issues.
- Framing follow-up intensity: a HAS-BLED ≥3 means tighter follow-up and risk-factor correction.
Not good for
- Deciding anticoagulation by itself. Stopping or withholding OAC based only on HAS-BLED is bad practice and contradicts guidelines. Stroke prevention decisions hinge on stroke risk (e.g., CHA₂DS₂-VASc) + shared decision-making, with bleeding risks mitigated where possible.
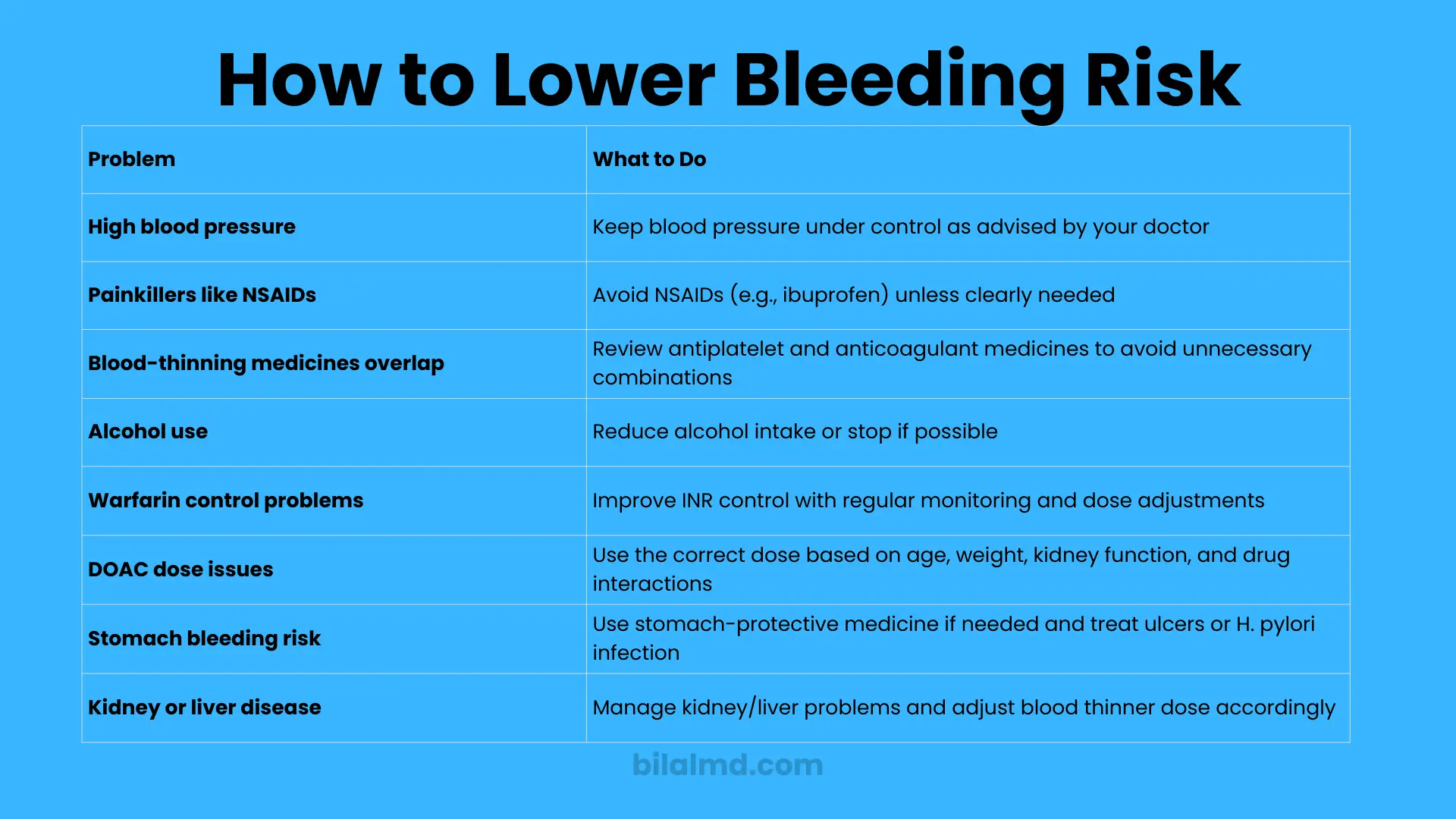
How to actually lower bleeding risk
If your HAS-BLED score is high, you don’t shrug you fix what you can:
- Control blood pressure (target per guideline/clinician advice; uncontrolled SBP is literally 1 point).
- Stop unnecessary NSAIDs and review antiplatelet therapy; avoid duplicate antithrombotics unless there’s a compelling indication and a clear stop date.
- Trim alcohol below risk-thresholds.
- On warfarin? Improve time-in-therapeutic range (education, dosing protocols, anticoagulation clinic).
- On DOACs? Use correct dose for age/weight/renal function and check drug interactions.
- GI risk: consider gastroprotection where appropriate; treat H. pylori/ulcer disease.
- Renal/liver disease: optimize management and adjust anticoagulant choices/doses accordingly.
These actions are exactly why the score exists: to identify and address modifiable bleeding risks.
HAS-BLED vs ORBIT vs ATRIA what if tools disagree?
- In head-to-head comparisons, ORBIT doesn’t reliably outperform HAS-BLED in anticoagulated AF populations; some datasets show similar or slightly better categorization for intracranial hemorrhage with HAS-BLED. Don’t overthink it, pick one validated method and use it consistently, focusing on risk-factor correction.
Worked example
A 72-year-old with hypertension, prior TIA, on warfarin with labile INR, and taking ibuprofen for knee pain:
- E (≥65) = 1
- H (BP often 170s) = 1
- S (TIA) = 1
- L (labile INR) = 1
- D (NSAID) = 1
Total = 5 → high bleeding risk; observed 1-yr bleeding ~12.5% in the original cohort. Priority actions: control BP, stop NSAID/consider alternatives, fix INR control or consider DOAC if appropriate, tighten follow-up. Anticoagulation decision still follows stroke risk and shared decision-making not HAS-BLED alone.
FAQs
What is a “good” HAS-BLED score?
Zero is best. 1–2 is moderate. ≥3 is high and demands risk-factor clean-up and closer monitoring. That does not automatically mean “no anticoagulant.”
Is a HAS-BLED of 3 dangerous?
It flags higher bleeding risk; in the original study, risk climbed notably from 3 upward. Use it as a to-do list for fixing risk factors, not a reason to abandon stroke prevention.
Does HAS-BLED apply to DOACs (apixaban, rivaroxaban, etc.) or only warfarin?
It was created in an era with much warfarin use, but it’s still used broadly. One component (Labile INR) is warfarin-specific; for DOAC users, that point is usually 0. The rest still matter (BP, drugs, alcohol, renal/liver disease, prior stroke/bleed, age).
What does “labile INR” actually mean?
Poor time-in-therapeutic range on warfarin (commonly TTR <60–65%). If your TTR is chronically low, your bleeding and stroke risks can worsen; fix adherence, monitoring, interactions or consider switching when appropriate.
Can I calculate HAS-BLED myself?
You can add up points, yes. But do not self-adjust or stop meds without a clinician; the score is not medical advice. It’s a nudge to fix risks (BP, alcohol, NSAIDs) and to talk with your clinician about safer regimens.
How often should HAS-BLED be reassessed?
At baseline and periodically because bleeding risk is dynamic. After any medication change (e.g., starting an NSAID) or clinical change (renal function, BP), reassess. High scores should trigger more frequent follow-up.
Which is “better” HAS-BLED or ORBIT?
There’s no consistent winner; studies are mixed. The decisive move isn’t the brand of score it’s correcting modifiable risks you uncover. If you pick one, use it consistently.
Does HAS-BLED replace CHA₂DS₂-VASc?
No. CHA₂DS₂-VASc estimates stroke risk; HAS-BLED estimates bleeding risk. You need both sides of the equation to make a rational anticoagulation plan. Guidelines are crystal-clear on this separation.
My HAS-BLED is 4. Should I stop apixaban?
Not automatically. First, attack modifiable risks (BP, drugs, alcohol). Then weigh your stroke risk and discuss options (dose appropriateness, PPI if GI risk, avoid NSAIDs/dual antiplatelets, closer follow-up). Stopping OAC solely for a high HAS-BLED score contradicts guidelines.
Where can I check the components if I forget them?
Any reputable clinical calculator lists them clearly (e.g., MDCalc) and mirrors the original publication. Still, decisions belong with your clinician.
Disclaimer
This article is educational. The HAS-BLED calculator helps you find and fix bleeding risks; it’s not a substitute for clinical judgment, diagnosis, or individualized treatment. Medication decisions especially starting, stopping, or switching anticoagulants must be made with a qualified clinician using your full medical history, current meds, labs, and preferences.
Resources
- Original derivation: Pisters et al., HAS-BLED, CHEST 2010 (Euro Heart Survey), includes observed 1-year bleeding rates by score.
- US guideline stance: 2023 ACC/AHA/ACCP/HRS AF guideline use bleeding scores to identify and modify risk, not to deny OAC.
- ESC stance: 2020 ESC AF guideline perform structured bleeding-risk assessment (e.g., HAS-BLED); high scores prompt closer review; don’t avoid OAC solely on estimated bleeding risk.
- Comparative performance: ORBIT vs HAS-BLED in anticoagulated AF; mixed results, no consistent superiority.