Use the DAPT Score Calculator to quickly estimate whether continuing dual antiplatelet therapy (DAPT) beyond 12 months may offer net benefit for you. Enter your clinical details below and review the result then read on to understand what it means and how to act.
DAPT Score Calculator
Estimate the potential net benefit of extended dual antiplatelet therapy after PCI. Educational use only.
Sources (for context): DAPT score derivation and validation studies, for example Mauri et al, N Engl J Med 2014 and Yeh et al, J Am Coll Cardiol 2016.
Disclaimers: This calculator is for education only and does not replace clinician judgement. Decisions on DAPT duration must consider bleeding and ischemic risk, stent type, and patient preferences.
Explore more heart calculator:
DAPT Score Calculator: How It Works and Why It Matters
What is the DAPT score?
The DAPT Score is a validated clinical tool designed to help clinicians and patients assess the trade-off between ischemic risk (heart attack, stent thrombosis) and bleeding risk when considering extended dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor) beyond 12 months after a percutaneous coronary intervention (PCI) with stent placement.
Simply put: After a stent, longer DAPT reduces ischemic events but increases bleeding. The DAPT score helps you estimate which side dominates for a given patient. In the original derivation, a score ≥ 2 indicated net benefit for prolonged DAPT, while a score < 2 suggested shorter or standard duration might be safer.
Why it matters
In modern cardiology, striking a balance between bleeding and ischemic risk is crucial. The DAPT score is among the first tools to uncouple those risks, letting clinicians personalise therapy rather than a one-size-fits-all. If you just continue DAPT indefinitely without reason, the bleeding risk rises. If you stop too early, you raise the chance of stent issues or myocardial infarction. This tool helps you make an informed decision.
Who the score applies to
Typically the score applies to patients who:
- Have undergone PCI with stent(s) and completed ≥12 months of DAPT without major bleed or ischemic event.
- Are not on chronic oral anticoagulation (which changes the calculus).
- Want to evaluate whether to continue DAPT beyond 12 months (or switch to monotherapy).
If you’re still within the first year post-PCI, or have recent major bleed or anticoagulant therapy, the DAPT score may be less applicable.
How the score is calculated
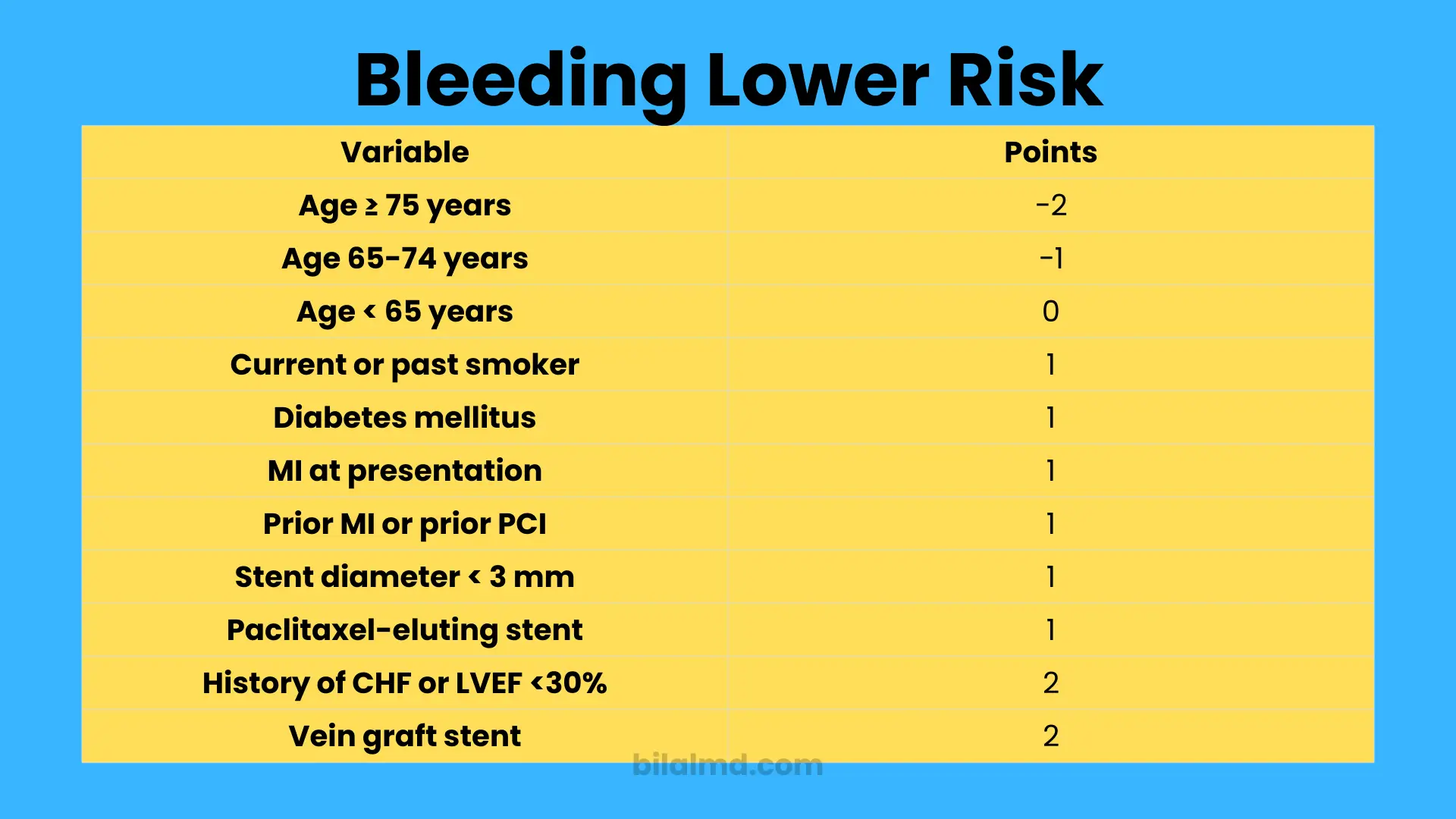
The DAPT score uses nine clinical/procedural variables. In brief:
| Variable | Points |
|---|---|
| Age ≥ 75 years | −2 |
| Age 65-74 years | −1 |
| Age < 65 years | 0 |
| Current or past smoker | +1 |
| Diabetes mellitus | +1 |
| MI at presentation | +1 |
| Prior MI or prior PCI | +1 |
| Stent diameter < 3 mm | +1 |
| Paclitaxel-eluting stent | +1 |
| History of CHF or LVEF <30% | +2 |
| Vein graft stent | +2 |
When added, the total score ranges from −2 to +10.
Interpreting the result
- Score ≥ 2 → Higher ischemic risk relative to bleeding risk → Prolonged DAPT may offer net benefit.
- Score < 2 → Bleeding risk may outweigh ischemic benefit → Standard or shorter DAPT may be appropriate.
Keep in mind: It’s a decision‐support tool, not a treatment mandate. Clinical judgment remains paramount.
Limitations to know
- The original study excluded patients who had major bleeding or ischemic events during the first 12 months. Applying it outside that population may reduce accuracy.
- External validation studies show moderate discrimination; the score is helpful but not perfect.
- The score doesn’t account for some newer stent types, newer antiplatelet drugs, or changing real-world populations.
- Always integrate patient preferences, comorbidities (renal disease, frailty), and newer guideline updates.
Practical steps after calculating
- Complete the calculator: Input your age, smoking status, diabetes, prior MI/PCI, stent size, stent type, CHF/LVEF, vein graft stenting, etc.
- Review the result: Note your score and the recommended direction (prolong vs standard duration).
- Discuss with your cardiologist: Bring the score into the conversation ask how your other bleeding and ischemic risk factors (renal function, frailty, medications) affect decision-making.
- Plan a timeline: If prolonged DAPT is indicated, clarify how long beyond 12 months, what antiplatelets will be used, and how bleeding risk will be monitored. If standard duration is advised, ask when to switch to single antiplatelet therapy and how to monitor for ischemic risk.
- Reassess periodically: Your risk profile changes age, new comorbidities, bleeding events, stent complications so periodic reassessment is wise.
FAQs
Here are frequently asked questions drawn from medical forums, Reddit discussions, Quora-type queries and social clinician dialogue:
Can I use the DAPT score immediately after my PCI (before 12 months)?
No. The DAPT score is designed after the first 12 months of uneventful DAPT (no major bleed/ischemic event). Using it earlier may lead to misleading benefit/bleed trade-offs.
If my DAPT score is ≥ 2, does that mean I must continue DAPT indefinitely?
Not at all. A score ≥ 2 suggests that prolonged DAPT may be beneficial, but “prolonged” usually means beyond 12 months for a defined period not indefinite. Duration should be individualized with your cardiologist.
My score is < 2. Does that mean I should stop DAPT right now?
No. It suggests that extended DAPT may offer less net benefit compared to bleeding risk. It doesn’t mean you stop right away it means you and your clinician should evaluate whether standard duration (12 months or guideline-recommended) is appropriate and plan the switch to mono-therapy with monitoring.
Does the score apply if I’m on oral anticoagulants too?
The original model excluded chronic anticoagulation patients. Additional risks apply when combining DAPT with anticoagulants, so the score’s accuracy may be diminished in that setting.
What about newer stents and P2Y12 inhibitors like ticagrelor/prasugrel? Does the score still hold?
Emerging data show the DAPT score remains a useful tool, but its performance may vary with newer stent types and modern antiplatelet regimens. Always interpret alongside current evidence.
If I had a minor bleed while on DAPT, can I still use the score?
If the bleed was major (requiring hospitalisation or transfusion) during the first 12 months, the DAPT score may not apply reliably. If it was minor, discuss with your clinician how that affects your bleeding risk separately.
What other scores should I know, besides the DAPT score?
Yes there’s the PRECISE‑DAPT Score which focuses more on bleeding risk (age, hemoglobin, renal function, prior bleed). It’s complementary to the DAPT score.
I’m older (≥75) with multiple comorbidities my score is low. Does that mean I should stop DAPT after 12 months?
A low score may lean toward shorter DAPT duration, but age/comorbidities increase bleeding risk and ischemic risk both. Clinical judgment is critical. Keep periodic review with your cardiologist.
Final word
The DAPT Score Calculator offers a streamlined, evidence-based way to evaluate whether extended dual antiplatelet therapy might offer net benefit for you. It should be used in conjunction with your clinician, not instead of them. Use the calculator as a launch point for informed discussion: Your history, stent type, comorbidities, bleed risk and preferences all matter.