Use this CPP calculator to compute cerebral perfusion pressure fast and correctly. Enter mean arterial pressure and intracranial pressure or central venous pressure, then review the step by step guide below to interpret results and see real clinical examples. This page also covers CPP calculation, normal and recommended targets, and common pitfalls that produce wrong numbers.
CPP Calculator
Cerebral Perfusion Pressure Calculator
Medical Disclaimer
This calculator is for educational and informational purposes only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always consult with qualified healthcare professionals for medical decisions. The calculations provided are based on standard formulas but individual patient care may require different approaches. This tool does not account for all clinical variables that may affect cerebral perfusion pressure management.
Explore more heart calculator:
CPP Calculator Guide
Everything you need to understand, calculate, and interpret cerebral perfusion pressure
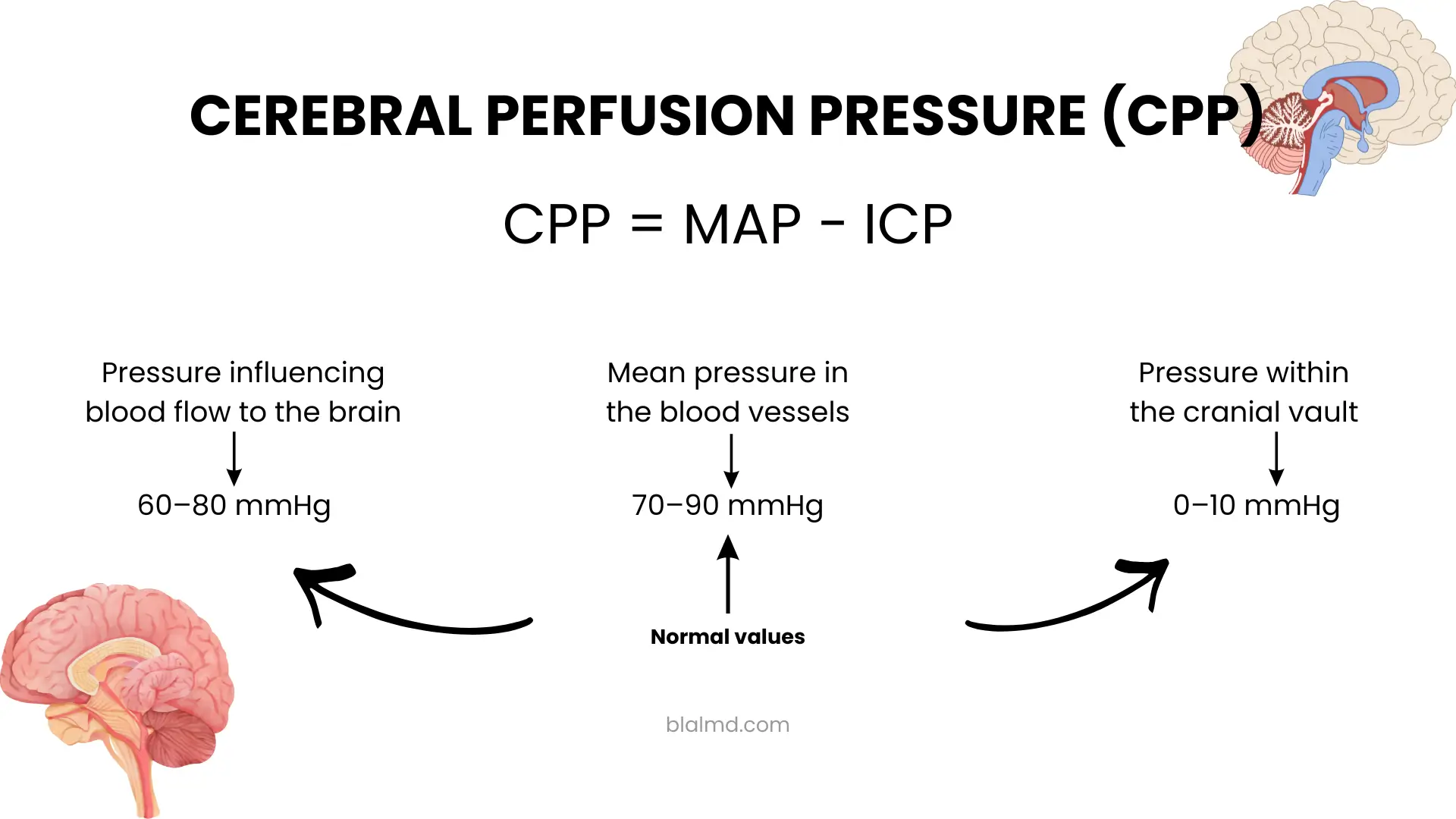
You asked for a straight answer with no fluff. Here it is. Cerebral perfusion pressure is the pressure gradient that drives blood flow through the brain. The working formula in day to day care is simple in words
CPP equals MAP minus ICP. If the central venous pressure is higher than the intracranial pressure then CPP equals MAP minus CVP. The goal is to know inflow pressure and outflow pressure and subtract the larger outflow from the inflow. That is what determines whether the brain is being perfused.
What values go into the CPP calculation
- MAP or mean arterial pressure. A quick bedside estimate uses the well known relationship
MAP equals diastolic pressure plus one third of pulse pressure. Pulse pressure is systolic minus diastolic. Automated monitors may compute MAP directly from the arterial waveform, but the one third method remains a widely cited estimate. - ICP or intracranial pressure. In a resting adult the normal ICP range is about 7to 15 millimeters of mercury. Sustained pressures above 20 to 25 are considered abnormal and typically trigger active therapy.
- CVP or central venous pressure. In some circumstances the venous pressure at the level of the brain outflow may exceed the ICP. When that happens you must subtract CVP from MAP rather than ICP.
The calculator on your page accepts MAP and either ICP or CVP, then performs the correct subtraction to produce CPP.
How to calculate CPP with examples
Example one
Systolic pressure 120 and diastolic pressure 75. Intracranial pressure 14.
First compute MAP. Pulse pressure is 120 minus 75 which is 45. One third of 45 is 15. Add that to diastolic 75 to get MAP 90.
Now compute CPP. CPP equals 90 minus 14 which is 76 millimeters of mercury. This is within commonly cited normal ranges.
Example two
Systolic pressure 98 and diastolic pressure 58. Intracranial pressure 22 during a spike.
Pulse pressure is 40. One third is about 13. Add to diastolic to get MAP about 71.
Now CPP equals 71 minus 22 which is 49. This is a concerning value in a brain injured patient and usually calls for action to raise MAP, reduce ICP, or both depending on the overall picture.
Example three where CVP matters
Systolic pressure 110 and diastolic pressure 70 so MAP is about 83. The patient is in a sitting or beach chair position with jugular venous congestion and measured CVP of 18 while ICP is only 12. Outflow is governed by the higher pressure which is CVP. CPP equals 83 minus 18 which is 65. Posture and venous factors can therefore lower CPP even when ICP looks acceptable.
What is a normal CPP and what should you target
In many references, a normal CPP for adults at rest is described as about sixty to eighty millimeters of mercury. In severe traumatic brain injury, the Brain Trauma Foundation suggests a therapeutic target between sixty and seventy. The exact best number within that band can vary with autoregulatory status and the entire clinical context. Your calculator is not a diagnostic tool and does not set a target for your patient. It simply provides the number so a clinician can decide whether to adjust MAP, ICP, or both.
Why CPP falls and what to do about it
CPP drops for two fundamental reasons: one, MAP decreases; two, ICP or CVP increases. The responses are equally fundamental
- Raise MAP with volume resuscitation and vasoactive agents when appropriate. Many critical care guidelines emphasize maintaining adequate systemic perfusion, often with MAP sixty five or higher in distributive states. This is not a one-size-fits-all rule in neurocritical care, but the principle that brain perfusion depends on systemic pressure is non-negotiable.
- Lower ICP with head elevation, sedation, osmotic therapy, cerebrospinal fluid drainage when available, and treatment of the cause of raised pressure. Most protocols intervene when ICP exceeds 22 for a sustained period.
- Address venous outflow problems such as high CVP, improper neck positioning, or adverse head elevation in operating room positions that can reduce the pressure gradient.
Common mistakes that break CPP calculation
- Using systolic pressure instead of MAP. CPP is not systolic minus ICP. Always compute MAP or take the monitor value.
- Ignoring CVP when it exceeds ICP. Outflow pressure is whichever of ICP or CVP is greater. Your calculation must subtract the larger one.
- Trusting a single number without context. Autoregulation, carbon dioxide, oxygenation, hematocrit, temperature, and sedation all influence cerebral blood flow at the same CPP. Use trends and the entire clinical picture.
Frequently asked questions
What is CPP in simple terms
It is the pressure that drives blood through the brain. At the bedside it is the difference between inflow and the larger of the two outflow pressures. Think of it as the usable pressure head that pushes blood across the cerebral circulation.
How do I calculate CPP
Compute or read MAP from the monitor. Obtain ICP from a monitor if present. If CVP is higher than ICP use CVP. Subtract the larger outflow from MAP. The calculator performs this step for you.
How do I calculate MAP
If the monitor does not show MAP, use the familiar estimate
MAP equals diastolic pressure plus one third of the difference between systolic and diastolic. Example, at 120 over 75, one third of 45 is 15 and MAP is 90.
What values are considered normal for ICP
In a resting adult an ICP around seven to fifteen is considered normal. Many protocols treat sustained pressures above twenty to twenty five.
What CPP should I aim for in severe traumatic brain injury
Authoritative guidance suggests a target between sixty and seventy. The precise point depends on autoregulation and the individual patient.
Can the calculator tell me whether the CPP is safe
No calculator can judge safety in isolation. A value of sixty five might be adequate in one patient and inadequate in another if autoregulation is impaired or if oxygen delivery is compromised. Use the number alongside examination, imaging, laboratory data, and neuromonitoring.
Why is my CPP low even though ICP is not very high
Look at MAP first. Hypotension will drop CPP even if ICP is normal. Check for venous factors as well, since high CVP or posture related hydrostatic effects can reduce the gradient.
Is the one third rule for MAP always correct
It is an estimate that works well enough for steady heart rates and regular pulse waves. Research versions of the formula that use different weightings also exist, and monitors may compute MAP from waveform integration. For transparent bedside math the one third rule remains acceptable.
Clinical safety notice
This content is educational. It does not replace clinical judgment or local protocols. A very low CPP in the setting of brain injury is a medical emergency. If your patient has a depressed level of consciousness, new focal deficits, or signs of herniation, activate emergency pathways immediately.
References
- StatPearls. Cerebral Perfusion Pressure. Definitions and physiology of CPP and its relationship with MAP.
- Blood Pressure physiology and MAP formula, StatPearls and peer reviewed literature on calculation methods.
- Normal ICP ranges and treatment thresholds, StatPearls point of care and reviews.
- Outflow pressure concept and choice of CVP when it exceeds ICP including posture related effects.
- Brain Trauma Foundation Fourth Edition Guidelines, target CPP sixty to seventy in severe traumatic brain injury.
Bottom line
Use the cpp calculator to compute CPP accurately. Confirm MAP, confirm the higher of ICP or CVP, subtract correctly, then treat the physiology that is lowering the gradient. A precise number is useful. A precise number interpreted in context is what changes outcomes.