Looking for a simple and reliable way to estimate prostate size and PSA density (PSAD)? Our Prostate Volume Calculator helps you quickly understand prostate measurements using commonly used clinical formulas, so you can feel more informed and confident when reviewing results or discussing them with a healthcare professional.
Why this calculator matters
Estimating prostate gland volume helps with BPH evaluation, biopsy decisions, and treatment planning. The most widely used clinical approach models the prostate as an ellipsoid and applies a constant derived from π/6 (~0.523). In practice, this is simplified to 0.52 and used across ultrasound and MRI workflows.
PSA density (PSAD) adds context to a raw PSA value by dividing PSA (ng/mL) by gland volume (cc). Historically, clinicians referenced 0.15 ng/mL/cc as a notable threshold; newer analyses suggest that when modern MRI quality is average or better, ≥0.20 may be a more appropriate trigger in MRI-negative patients. Always interpret PSAD within a full clinical assessment.
How the calculator works (and how to get the best result)
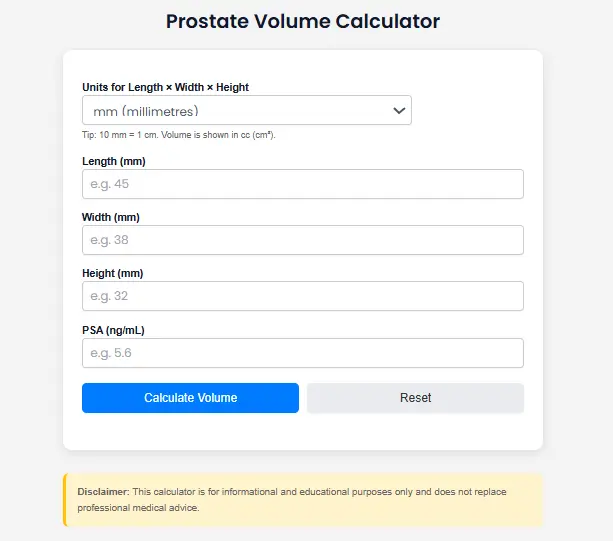
- Gather three dimensions from your imaging report (US/MRI/CT): Length × Width × Height.
- Enter them in mm or cm the tool converts mm → cm for you and add the PSA (ng/mL).
- The tool computes:
- Prostate Volume (cc) using the ellipsoid formula: L × W × H × 0.52.
- PSA Density (PSAD): PSA ÷ Volume (cc).
- See your results instantly and review the interpretation tips below.
Why ellipsoid? It’s quick, reproducible, and accepted for routine clinical use. Alternative “bullet-shape” formulas exist and may better fit certain gland shapes, but 0.52 remains the standard starting point for most calculators.
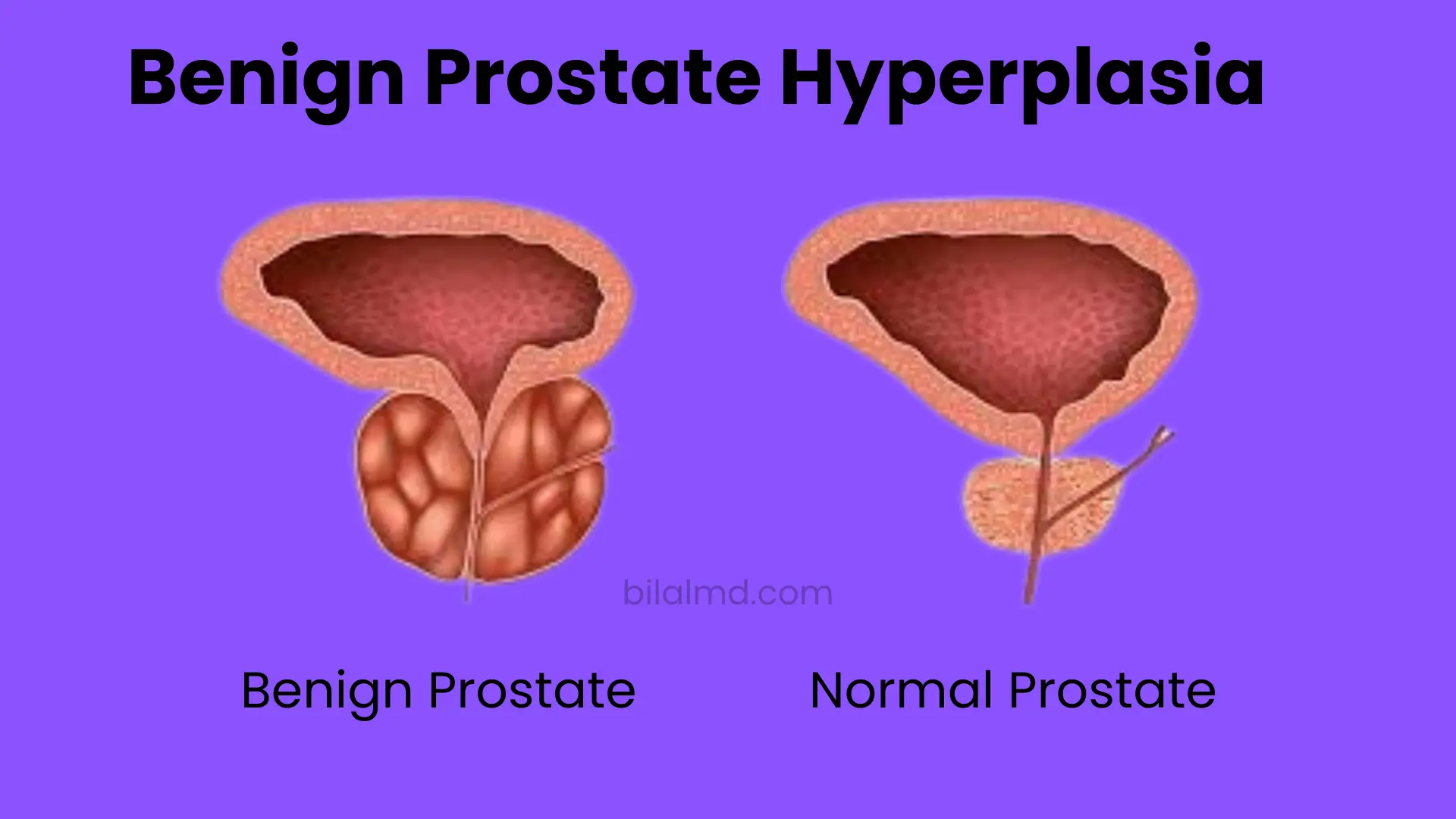
What counts as a “normal” prostate volume?
Published references often cite an upper limit of ~30 cc as normal on imaging, recognizing that volume gradually increases with age. In a large age-stratified cohort (50–80 y), mean prostate volume rose from ~24 cc to ~38 cc. Use age and clinical context when interpreting any single value.
Ultrasound vs MRI vs CT: which is most accurate?
- Ultrasound (TRUS/TAUS): Widely available; accuracy varies with technique and anatomy. Some studies find TRUS can under- or over-estimate volume; standardized methods reduce variability.
- MRI: Often shows better correlation with surgical specimen volume and may be preferred, especially for larger glands or when US and MRI disagree.
- CT: Can be used when MRI/US are unavailable; apply the same ellipsoid approach, but be mindful of slice thickness and reconstruction planes.
Example calculations (so you know what your numbers mean)
- Example A (Ultrasound in mm):
L = 45 mm, W = 38 mm, H = 32 mm → convert to cm → 4.5 × 3.8 × 3.2 × 0.52 = 28.4 cc.
If PSA = 1.4 ng/mL → PSAD = 1.4/28.4 = 0.049 ng/mL/cc. - Example B (MRI in cm):
L = 5.2 cm, W = 4.8 cm, H = 3.9 cm → 5.2 × 4.8 × 3.9 × 0.52 = 50.6 cc.
If PSA = 5.0 ng/mL → PSAD = 5.0/50.6 = 0.099 ng/mL/cc.
These examples show how the same PSA can imply different risk depending on gland size, underscoring why PSAD is clinically useful.
Quick interpretation guide (not medical advice)
- Volume: Many references consider ≈30 cc as a rough upper-normal on imaging; larger values are common with age and BPH.
- PSAD: Historic cutoffs around 0.15 ng/mL/cc are frequently cited; recent MRI-era analysis argues ≥0.20 may be more appropriate in MRI-negative men. Discuss any threshold with your clinician.
Pro tips to improve measurement cnsistency
- Check units: Many reports list mm; convert to cm before calculating.
- Repeat when unsure: If the gland is irregular (e.g., large median lobe), duplicate measurements or confirm on MRI.
- Document and compare: Track volume over time; prostate size typically increases with age, so looking at trends is more informative than a single value.
FAQs
How to calculate prostate volume?
Use the ellipsoid method: Volume (cc) = Length × Width × Height × 0.52 (dimensions in cm). This is the most commonly accepted, fast, and reproducible approach in radiology and urology.
How to calculate prostate volume in ultrasound?
Measure three orthogonal diameters (typically width on axial; length and height on mid-sagittal), convert to cm, then apply L × W × H × 0.52. If your report lists mm, divide by 10 first. Technique and probe pressure can affect results.
How do you calculate prostate volume (general)?
Same method across US/MRI/CT collect three diameters, convert to cm, calculate L × W × H × 0.52. For atypical shapes, some researchers evaluate “bullet-shape” coefficients (≈0.65) but ellipsoid remains the standard.
How to calculate prostate volume by ultrasound (step-by-step)?
- Obtain axial width (transverse);
- Obtain mid-sagittal length and height (AP);
- Convert to cm;
- Compute L × W × H × 0.52;
- If repeated measures vary, average two consistent reads.
How to calculate prostate volume on ultrasound?
Repeat the same ellipsoid steps; keep calipers consistent and avoid measuring peri-prostatic tissue. If a prominent median lobe complicates caliper placement, consider repeating measurements or using MRI for confirmation.
How to calculate prostate volume on CT scan?
Pick planes carefully (often width on axial; length and height on sagittal/coronal), convert to cm, and use ellipsoid 0.52. CT can be used when US/MRI aren’t available, but be mindful of slice thickness.
How to calculate volume of prostate ?
No matter the modality, use the three diameters in cm with 0.52. For select scenarios (e.g., very small glands), “bullet” approximations may slightly adjust results, but they are less commonly used in routine clinics.
What is a normal prostate volume?
On imaging references, ~30 cc is often cited as an upper-normal limit, but volume increases with age (e.g., mean ~24 cc at 50 rising to ~38 cc at 80 in one population study). Always interpret volume with symptoms and exam.
Is 40 cc enlarged?
Many sources consider >30 cc above typical adult “normal,” but “enlarged” isn’t a diagnosis by itself. Symptoms, uroflow, PSA, DRE, and imaging all matter. Discuss thresholds with your clinician.
What is PSA density (PSAD) and how do I use it?
PSAD = PSA ÷ prostate volume (cc). It contextualizes PSA by gland size. While 0.15 ng/mL/cc is commonly referenced, newer MRI-era analysis suggests ≥0.20 may be a better cut-point in MRI-negative men; clinicians individualize decisions.
Which is more accurate MRI or ultrasound for volume?
Both correlate with pathology, but MRI often shows better agreement, particularly in larger glands or when measurements disagree. If precision matters (e.g., surgical planning), MRI can help confirm.
Can I use this prostate gland volume calculator if my report lists mm?
Yes. Our calculator accepts mm or cm and converts automatically (10 mm = 1 cm) before applying 0.52.
Does the ellipsoid 0.52 ever change?
The constant comes from π/6 (~0.523). Some research explores different coefficients to better fit non-ellipsoid shapes (e.g., “bullet” ≈0.65), but 0.52 remains the everyday clinical default.
Can I compute PSAD if I only have PSA and one or two dimensions?
You need all three dimensions to estimate volume, then divide PSA by that volume. If dimensions are missing, ask the imaging provider for the full report.
References
- PSAD thresholds in MRI-negative cohorts; historical 0.15 vs suggested ≥0.20.
- Ellipsoid formula (0.52) for routine US/MRI volume estimation and general technique.
- MRI vs TRUS accuracy vs pathology; MRI often more consistent, especially in larger prostates.
- Normal volumes and age-related increase.