A pediatric dose calculator is one of the fastest and safest ways to convert mg per kg medication orders into accurate, defensible doses. When I was working in the clinic early on, I remember struggling with these calculations myself especially converting pounds to kilograms and turning milligrams into milliliters. Small mistakes felt easy to make, and that uncertainty can slow you down.
That experience is exactly why I created this guide and a dedicated pediatric dose calculator section for juniors. This guide walks through the exact math behind the calculator, highlights common pitfalls such as lb versus kg confusion and liquid mL conversions, and answers the real questions clinicians and parents ask every day. The goal is simple: make your dosing workflow faster, clearer, and more reliable, whether you are learning or practicing in a busy clinical setting.
The two dosing patterns you’ll see (and how the math works)
Most pediatric orders use one of two styles:
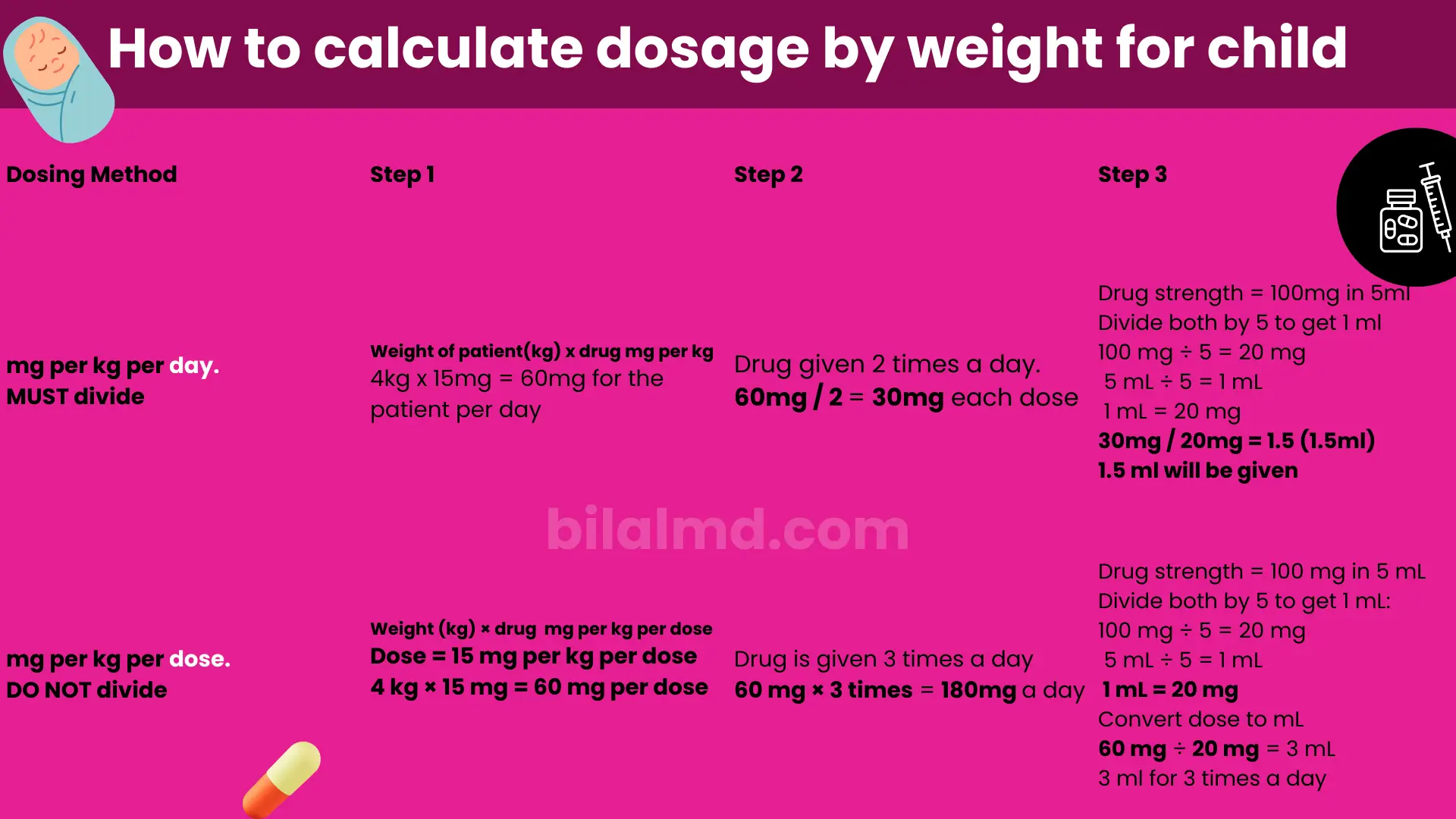
1️⃣ mg per kg per day divided qXh
(MUST divide)
Given
- Weight = 4 kg
- Dose = 15 mg per kg per day
- Frequency = q8h (3 times per day)
- Drug strength = 100 mg per 5 mL = 20 mg per mL
WHO format applied
mg per day
mg/day = weight × mg/kg/day
= 4 × 15
= 60 mg per day
mg per dose
mg/dose = mg/day ÷ doses per day
= 60 ÷ 3
= 20 mg per dose
mL per dose
mL/dose = mg/dose ÷ (mg/mL)
= 20 ÷ 20
= 1 mL
Final instruction
👉 Give 1 mL every 8 hours (3 times daily)
2️⃣ mg per kg per dose qXh
(DO NOT divide)
Given
- Weight = 4 kg
- Dose = 15 mg per kg per dose
- Frequency = q8h (3 times per day)
- Drug strength = 100 mg per 5 mL = 20 mg per mL
WHO format applied
mg per dose
mg/dose = weight × mg/kg/dose
= 4 × 15
= 60 mg per dose
mg per day
mg/day = mg/dose × doses per day
= 60 × 3
= 180 mg per day
mL per dose
mL/dose = mg/dose ÷ (mg/mL)
= 60 ÷ 20
= 3 mL
Final instruction
👉 Give 3 mL every 8 hours (3 times daily)
Either way, you must confirm the drug’s max single and max daily dose in an authoritative reference before finalizing.
Small steps that prevent big errors
- Chart weight in kilograms only. Wrong-unit entries (lb vs kg) are a well-documented source of pediatric dosing errors; multiple safety bodies recommend kg-only documentation.
- Give liquids in mL, not teaspoons. Use an oral syringe or marked cup and convert doses to mL per dose from the product’s mg/mL.
- Know typical over-the-counter (OTC) strengths. In the U.S., children’s acetaminophen liquids are 160 mg/5 mL; standard dosing is 10–15 mg/kg/dose every 4–6 hours (respect max daily dose per your local guidance).
Quick worked examples
Example A — Order written as mg/kg/day ÷ frequency
Order: 30 mg/kg/day, q12h (2 doses/day)
Weight: 6 kg Concentration: 31.25 mg/mL
- mg/day = 6 × 30 = 180 mg/day
- mg/dose = 180 ÷ 2 = 90 mg/dose
- mL/dose = 90 ÷ 31.25 = 2.88 mL
- Total daily volume = 180 ÷ 31.25 = 5.76 mL
Example B — Order written as mg/kg/dose
Order: 10 mg/kg/dose, q6h (4 doses/day)
Weight: 12 kg Conc: 100 mg/5 mL (= 20 mg/mL)
- mg/dose = 12 × 10 = 120 mg
- mg/day = 120 × 4 = 480 mg/day
- mL/dose = 120 ÷ 20 = 6 mL
These mirror the calculator’s logic and the WHO convention of presenting total daily dose ÷ frequency when orders are per day.

What clinicians and parents ask online (stand-alone FAQs)
Each question below is phrased the way people actually search for it (from Reddit/parenting and professional threads, plus common “People also ask” patterns), with concise answers you can use at the bedside. Where a drug is mentioned, always check your local monograph for exact limits.
How to calculate pediatric dose
Use kg, decide if the order is mg/kg/day or mg/kg/dose, apply the frequency, then convert mg→mL using the product’s mg/mL. A pediatric dose calculator automates these steps and reduces arithmetic slips.
How do you calculate pediatric doses
For mg/kg/day, compute mg/day then divide by doses/day for mg/dose; for mg/kg/dose, compute mg/dose then multiply by doses/day for mg/day. Convert to mL per dose from mg/mL and confirm max single/max daily.
How to calculate dose in pediatrics
Record weight in kilograms only and express liquids in mL, not teaspoons; both steps are emphasized in pediatric safety guidance.
How to calculate doses in pediatrics
Follow: kg × mg/kg → mg, apply q24–q4 frequency, and convert to mL (mg ÷ mg/mL). This is the core of pediatric dose computation used across guidelines.
How to calculate pediatric safe dose range
Look up the regimen’s min–max mg/kg and absolute maxima in your formulary, then cap outputs in the pediatric dose calculator accordingly.
What are the 4 methods used in calculating pediatric doses
The common approaches you’ll see are weight-based (mg/kg), age-bands, body-surface-area (mg/m²) for select drugs, and fixed dosing in older adolescents for some agents. Always default to the specific monograph.
How to calculate a pediatric dose
Multiply kg × mg/kg, apply frequency for mg/dose or mg/day, then convert to mL/dose via mg/mL. Verify against max single/daily limits.
How to calculate amoxicillin dose for pediatrics
High-dose amoxicillin for AOM is often 80–90 mg/kg/day divided BID; compute mg/day, split into two doses, and convert to mL from the suspension strength. (Always confirm local limits.)
How to calculate augmentin dose pediatric
Many protocols mirror amoxicillin (e.g., 80–90 mg/kg/day divided q12h by the amoxicillin component) and set maximums—check yours, then use the peds dose calculator to convert to mL per dose.
How to calculate azithromycin dose for pediatrics
Commonly 10 mg/kg on day 1, then 5 mg/kg/day on days 2–5 for some infections; enter the day-specific mg/kg, compute mg and mL from mg/mL, and verify maxima by indication.
How to calculate ceftriaxone dose in pediatrics
A frequent pattern is 50–75 mg/kg/day for many infections and 100 mg/kg/day for meningitis; pick per day or per dose as your source states and apply the frequency (e.g., q24 vs q12 for meningitis).
How to calculate pediatric antibiotic dose
If the order reads mg/kg/day ÷ qXh, compute mg/day then split by the number of doses; if mg/kg/dose, compute mg/dose then total the day. Convert to mL using mg/mL.
How to calculate pediatric dose by weight
The core step is kg × mg/kg. The pediatric dose calculator then handles frequency and mg→mL conversion safely.
How to calculate pediatric dose formula
There isn’t one universal formula; apply the drug-specific mg/kg or mg/m² statement, the frequency, and maxima. The calculator implements both mg/kg/day and mg/kg/dose paths.
How to calculate pediatric dose of amoxicillin
If it’s written mg/kg/day divided BID, use per day with q12h; if mg/kg/dose, use per dose and multiply by your daily frequency. Always check the max daily dose.
How to calculate pediatric tylenol dose (acetaminophen)
Use 10–15 mg/kg/dose q4–6h and the liquid’s 160 mg/5 mL to convert to mL per dose; respect the max daily dose per local guidance.
Pro tips that boost safety
- Kilograms only in EHR/e-Rx; wrong-unit entries are a classic failure mode.
- mL-only dosing devices for caregivers; avoid spoons.
- Show both mg and mL in your notes/prescription, with the product’s mg/mL strength. (Acetaminophen liquid 160 mg/5 mL is a common U.S. standard.)
- Link back to the tool from your dosing articles and case write-ups; users (and search engines) love a tight loop between pediatric dose calculator, pediatric dose computation examples, and deeper guidance.
Keep going
- Read the main guide + use the live tool: Pediatric Dose Calculator
- Next up on our blog: practical case walkthroughs (amoxicillin AOM, acetaminophen fever, ceftriaxone meningitis dosing)—each with mg/kg math and mL per dose conversions.
References & further reading
- WHO Expert Meeting: present regimens as total daily dose divided by frequency (q12h, q8h, etc.).
- AHRQ PSNet & EMS resources on lb↔kg mistakes and weight documentation best practice.
- AAP HealthyChildren acetaminophen dosing and U.S. liquid concentration standard (160 mg/5 mL).
- MedlinePlus overview on acetaminophen dosing.
- UCSF pediatric antimicrobial dosing examples and frequency patterns.
- HSSIB/NHS patient-safety report on weight-based prescribing errors in children.
Disclaimer: This blog supports—but does not replace—clinical judgment. Always verify drug-specific doses, ranges, and maxima in your local formulary; adjust for age, organ function, and indication; and consult pharmacy for complex cases.