If you’re searching for “LDL calculator,” “LDL cholesterol calculated,” or simply “how do you calculate LDL”, you’ve already realized something: not all calculated LDL results are equally reliable. The equation your lab or app chooses matters especially when triglycerides (TG) are elevated or LDL-C is low. Below is the practical, evidence-based guide to LDL calculation
What does “calculated LDL” actually mean?
Most lipid panels report LDL-C as calculated, not measured directly. The lab plugs Total Cholesterol (TC), HDL-C, and Triglycerides into a formula and outputs LDL cholesterol calculated. That’s faster and cheaper than a direct assay, but accuracy depends on the equation and the patient’s TG range.
The three equations that matter
1) Friedewald: the classic baseline
- Formula (mg/dL):
LDL-C = TC − HDL-C − (TG/5) - Use when: TG is modest (historically <400 mg/dL) and LDL is not very low.
- Limitations: Built on a small 1972 dataset; it assumes VLDL ≈ TG/5, which breaks with higher TG and at low LDL. Expect underestimation and category mistakes in those scenarios.
2) Martin/Hopkins: adjustable factor (better across typical ranges)
- What’s new: Replaces the fixed “/5” with a data-driven factor that varies by TG and non-HDL strata, improving accuracy at lower LDL and moderate-to-high TG.
- Extended version: Validated up to TG 799 mg/dL using a 240-cell stratification.
- Evidence: Multiple validations show higher accuracy than Friedewald and strong performance across ranges.
3) Sampson-NIH (2020): top pick when TG is high
- Why it matters: Designed to perform well with TG 400–800 mg/dL, the trouble zone for Friedewald.
- Results: About 35% fewer LDL treatment-group misclassifications in hypertriglyceridemia vs Friedewald; solid in fasting and non-fasting states.
Bottom line: If you need one rule, use a modern equation (Sampson-NIH or Martin/Hopkins) when TG is elevated or LDL is low; Friedewald is fine only inside its comfort zone. That’s exactly how our LDL calculator behaves.
How our LDL calculator chooses the formula
- Auto-select logic:
- TG ≥ ~400 mg/dL: Prefer Sampson-NIH for better accuracy in this range (up to ~800 mg/dL).
- TG < 400 mg/dL or LDL near decision thresholds: Use Martin/Hopkins for improved precision at lower LDL.
- Fallback: If values clearly fit the original assumptions, we can compute Friedewald and display it with a method tag, but we still show the modern estimate first.
- Safety rails: If TG > ~800 mg/dL, we flag the output and recommend a direct LDL-C test. That’s standard laboratory practice.
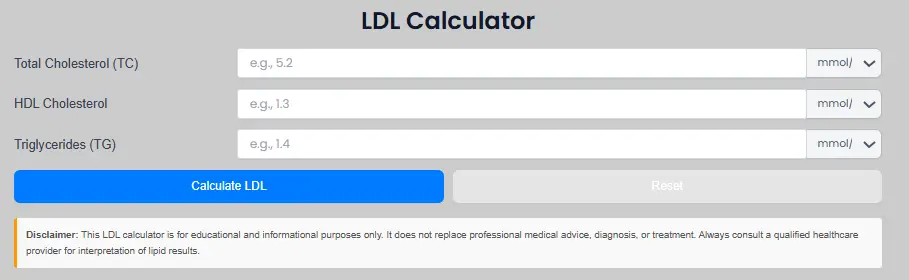
Step-by-step: calculate LDL, non-HDL, and the LDL: HDL ratio
- Enter your numbers (TC, HDL-C, TG).
- Choose units (mg/dL or mmol/L).
- Click Calculate. You’ll see:
- LDL cholesterol calculated (with the equation name).
- Non-HDL cholesterol (TC − HDL-C), which captures all atherogenic particles and is a robust secondary target when TGs are higher.
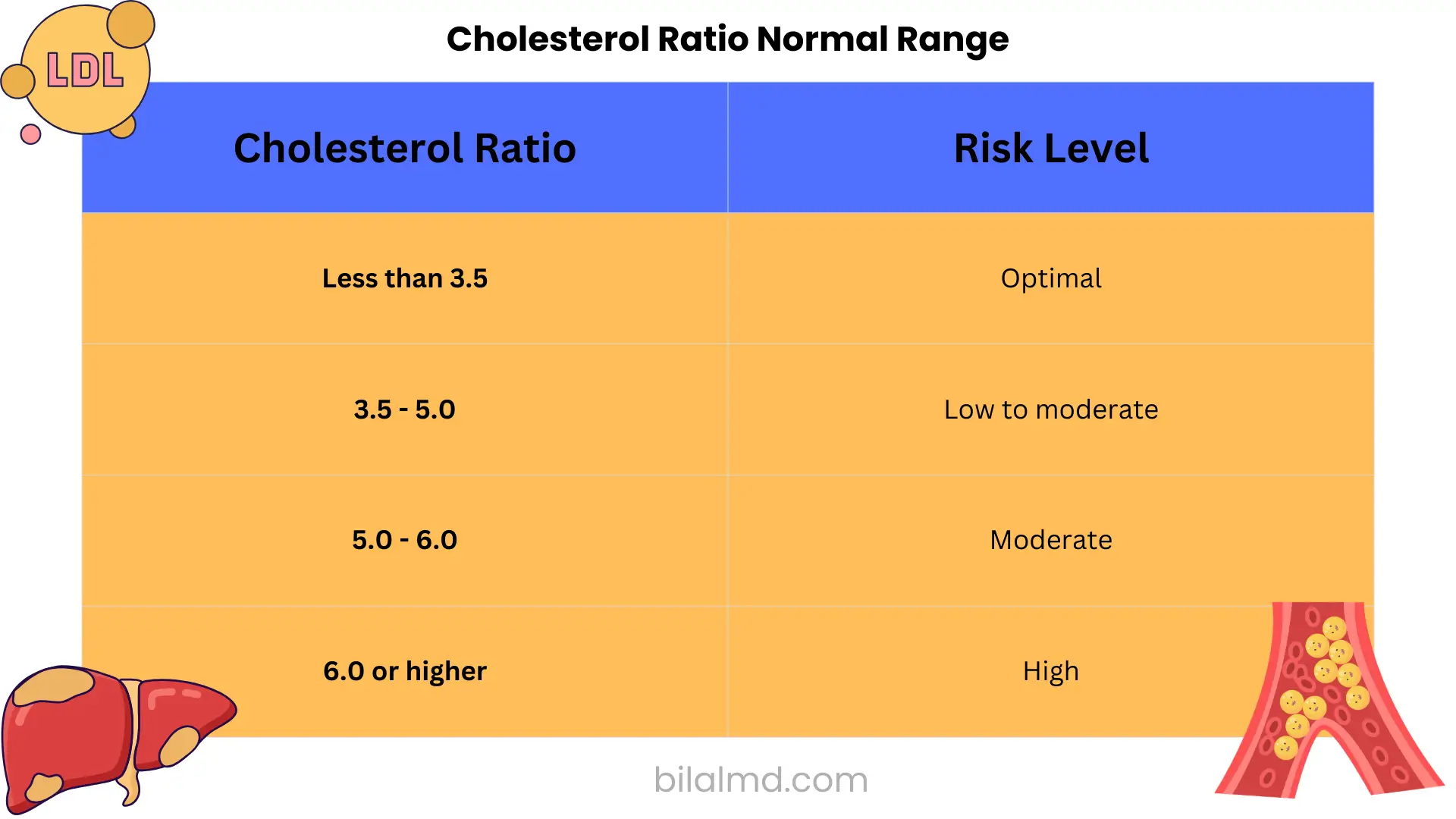
- LDL to HDL ratio (LDL-C ÷ HDL-C) for context only. Decisions should center on absolute LDL-C/non-HDL-C plus overall risk.
Why add non-HDL? It remains informative when TG fluctuate and is emphasized in many practice settings as a useful, easy-to-compute risk marker.
“How to calculate LDL?”
- How to calculate LDL / how do you calculate LDL / how to calculate LDL-C
Use TC, HDL-C, TG and a validated formula. Our tool auto-selects Sampson-NIH or Martin/Hopkins (and shows Friedewald when valid) to minimize misclassification. - How is LDL calculated / what is calculated LDL in a blood test
It’s an equation-based estimate, not a direct lab measurement. Accuracy changes with the equation, especially if triglycerides are high. - How to calculate LDL: HDL ratio
LDL:HDL = LDL-C ÷ HDL-C. Use it for context; don’t let it replace risk-based thresholds that drive treatment. - What is the LDL calculation?
Historically, Friedewald (TC − HDL − TG/5); now Martin/Hopkins and Sampson-NIH outperform it in many real-world lipid panels.
Fasting vs non-fasting: do you really need to fast?
Short answer: Not routinely. Multiple guidelines and consensus statements endorse non-fasting lipid profiles for most situations. If non-fasting TG ≥ ~400–500 mg/dL, repeat with fasting for clarity, and our calculator will tell you that.
Why our LDL calculator deserves your trust
- Evidence-based formulas: We implement Sampson-NIH (JAMA Cardiology 2020) and extended Martin/Hopkins (validated up to TG 799 mg/dL) so that calculated LDL stays accurate when it counts.
- Method transparency: Every result is labeled with the equation used.
- Guardrails for extremes: If TG are too high for any reliable LDL-C calculation, we flag the result and advise direct LDL-C mirroring modern lab practice.
- Non-fasting friendly: Our interface assumes non-fasting is often acceptable and prompts a fasting re-check only when appropriate.
👉 Calculate now: Open the LDL calculator
Quick reference: formulas, ranges
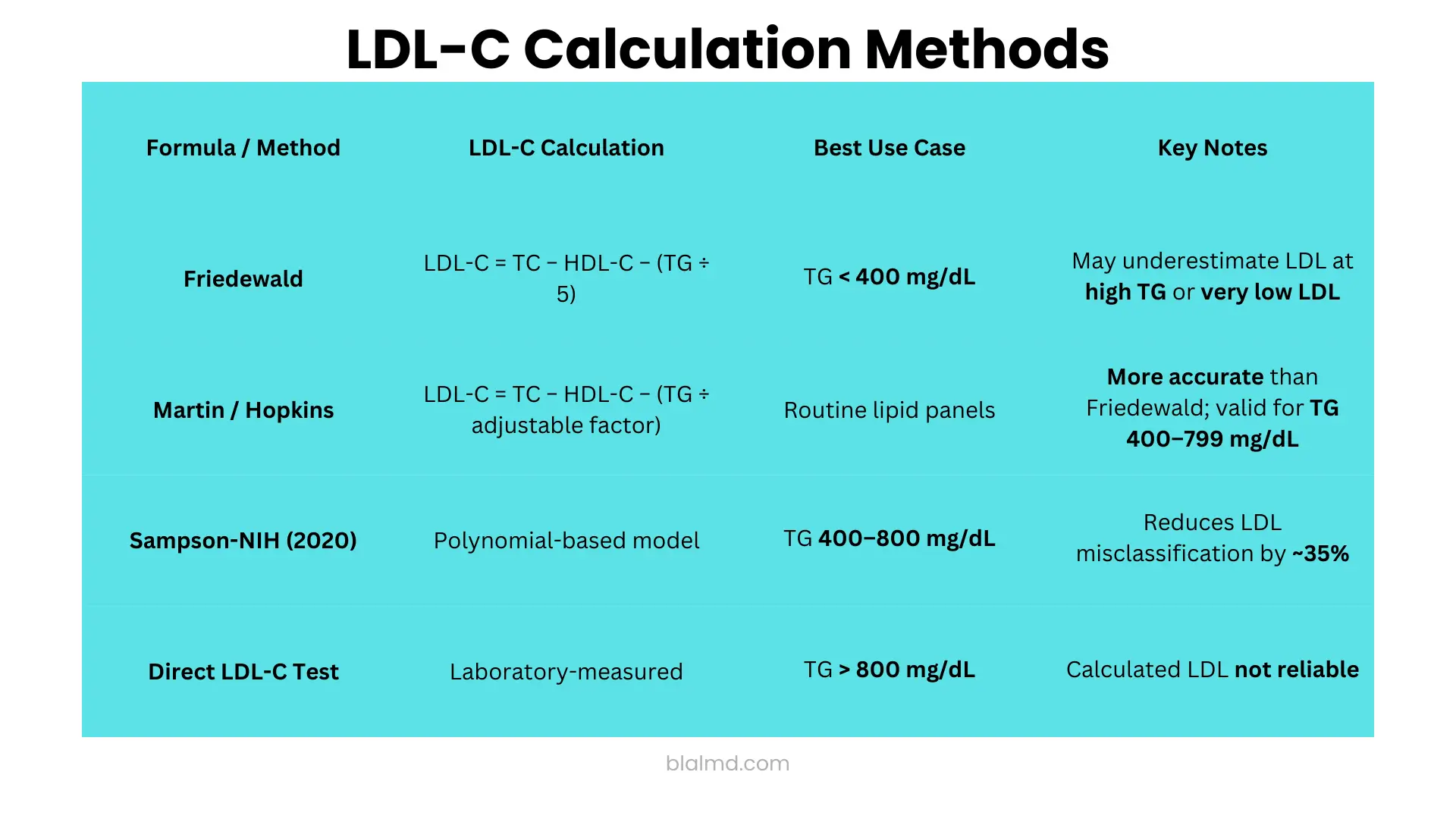
- Friedewald (mg/dL):
LDL-C = TC − HDL-C − TG/5
OK when TG < 400 mg/dL, but can underestimate at high TG or low LDL. - Martin/Hopkins:
LDL-C = TC − HDL-C − (TG ÷ adjustable factor)
More accurate across typical outpatient panels; extended for TG 400–799 mg/dL. - Sampson-NIH (2020): Polynomial-style model that cuts misclassification ~35% in TG 400–800 mg/dL compared with Friedewald.
- When TG > ~800 mg/dL: Do not trust a calculated LDL; order a direct LDL-C (our page will warn you).
FAQ
Is “calculated LDL” the same as direct LDL?
No. Calculated LDL uses equations; direct LDL-C measures it in the lab. Calculated is fine most of the time if you use the right equation for the TG range.
Can I calculate LDL from just total and HDL?
No you need triglycerides to estimate VLDL-C in all common equations. Use a full lipid panel.
Should I rely on the LDL:HDL ratio calculator?
Use it for context; therapy decisions are based on absolute LDL-C/non-HDL-C and overall risk, per major guidelines.
Is calculated LDL the same as direct LDL?
No. Calculated LDL-C is derived from TC, HDL-C, and TG using equations (Friedewald, Martin/Hopkins, Sampson-NIH). Direct LDL-C is an assay. Calculated LDL can underestimate when TG are high or LDL is low; modern equations reduce (not eliminate) that error. Direct assays aren’t perfect either. Use calculated LDL with a modern formula and reserve direct LDL when TG are extreme or flagged.
Which LDL calculation is most accurate?
In routine panels, Martin/Hopkins outperforms Friedewald, especially at low LDL or higher TG. For TG ~400–800 mg/dL, Sampson-NIH is usually the best choice and is increasingly recommended by labs.
Do I need to fast for a lipid panel with calculated LDL?
Not routinely. Non-fasting lipids are acceptable for most people. If a non-fasting TG ≥ ~400 mg/dL, repeat a fasting panel. Your calculator page should surface this guidance.
What is the Friedewald formula and when does it fail?
LDL-C = TC − HDL-C − (TG/5) (mg/dL). Valid mainly if TG < 400 mg/dL and LDL isn’t very low. It often underestimates LDL at higher TG or low LDL.
What’s different about the Martin/Hopkins equation?
It replaces the fixed “/5” with a data-driven adjustable factor based on TG and non-HDL strata, boosting accuracy; an extended version works up to TG ≈ 799 mg/dL.
What does the Sampson-NIH equation improve?
It reduces LDL misclassification when TG are elevated (≈400–800 mg/dL) versus Friedewald and performs well fasting or non-fasting hence many labs prefer it.
Can I calculate LDL without triglycerides?
No. All common LDL-C equations require TG to estimate VLDL-C. Without TG, you cannot compute calculated LDL.
What’s “non-HDL cholesterol,” and should I see it with my result?
Non-HDL-C = TC − HDL-C. It captures all atherogenic apoB-containing particles and is especially helpful when TG are higher. Show it alongside calculated LDL.
Are LDL:HDL ratios useful?
LDL:HDL = LDL-C ÷ HDL-C. It’s context only. Treatment decisions rely more on absolute LDL-C/non-HDL-C and overall risk.
Is calculated LDL reliable at very high triglycerides?
Once TG approach/ exceed ~800 mg/dL, any calculation becomes shaky flag it and consider direct LDL-C or clinician follow-up.
Why do different calculators give different answers?
Because they use different equations (Friedewald vs Martin/Hopkins vs Sampson-NIH), each handling TG and low LDL differently. Your page should label the method used.
Are direct LDL assays always better than calculated LDL?
Not always. Some direct methods can be inaccurate in high TG or mixed dyslipidemia. Modern calculated methods may match or exceed them in specific ranges. Use either with clinical context.
What LDL number is considered “high”?
Cut-points depend on risk. Many summaries still show LDL ≥190 mg/dL as clearly high in primary prevention; very-high-risk ASCVD targets are <70 mg/dL (or lower per clinician judgment). Keep interpretation risk-based.
Can I use non-fasting results to start treatment?
Yes guidelines allow it, with the caveat that non-fasting TG can run 10–30 mg/dL higher; repeat fasting if TG are high or results are borderline for a therapy decision.
Why does your calculator show multiple LDL values?
Transparency. We prioritize Sampson-NIH or Martin/Hopkins (depending on TG), but also display Friedewald when valid so clinicians can compare and decide.
The takeaway
If a page uses only the 1972 Friedewald math and calls it a day, it can mislead exactly when precision matters high TG or low LDL. Our LDL calculator auto-selects Sampson-NIH or Martin/Hopkins, labels the method, shows non-HDL, and warns you when a direct LDL-C is the right next step. That’s how LDL cholesterol calculated should work in 2025.
Ready? Use the LDL calculator now and get a clinically sound, clearly explained result in seconds.
Sources
- ACC explainer on LDL-C estimation and Friedewald limitations.
- Sampson-NIH equation performance (JAMA Cardiology & PubMed).
- Extended Martin/Hopkins validation up to TG 799 mg/dL; large comparative studies.
- Non-fasting lipid guidance (ACC/AHA, EAS consensus, reviews).
- Lab practice on TG > 800 mg/dL requiring direct LDL-C.