If you’re monitoring warfarin, the number that matters most is INR. Below is a practical guide what INR is, how to calculate it, why it fluctuates, and evidence-based answers to the most common community questions
What is INR (and why not just PT)?
INR standardizes the Prothrombin Time (PT) across different labs and reagents using the ISI (International Sensitivity Index). The core formula is: INR = (Patient PT / Control PT) ^ ISI
Standardization is needed because thromboplastins have different sensitivities (ISI). INR normalizes these differences so results are comparable across labs.
Typical target ranges (quick reference)
- Not on anticoagulants: ~0.8–1.2.
- Most warfarin indications: 2.0–3.0.
- Mechanical valves: target depends on valve type & position; e.g., bileaflet/current-gen single-tilting disk AVR often 2.5; mitral mechanical commonly 3.0; On-X AVR may allow 1.5–2.0 with ASA after 3 months (clinician-directed). Always follow patient-specific guidance.
- ⚠️ High INR management is protocol-based. As a general reference, expert resources advise holding doses and, for very high INR without bleeding (e.g., >10), giving oral vitamin K; always follow your clinician/local protocol.

How INR is calculated
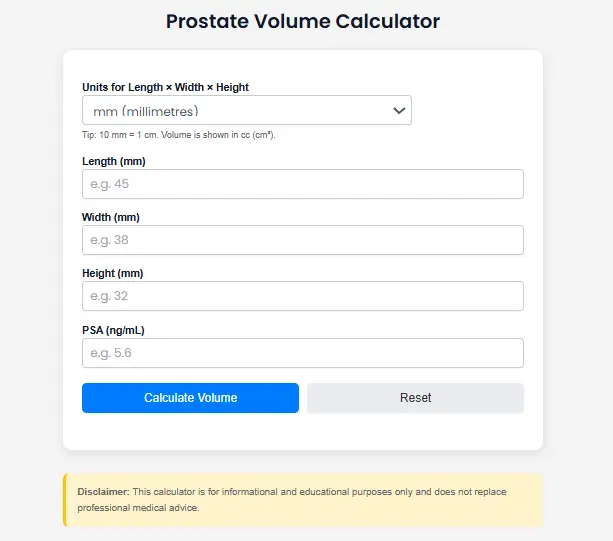
INR depends on three inputs: Patient PT, Control PT, and ISI. Instead of doing it by hand, use our quick tool. The tool displays a result and simple interpretation bands consistent with common clinical targets above.
Why INR moves: the big drivers
- Vitamin K intake (diet) changes → more Vit K can lower INR; less can raise INR consistency is key.
- Medications & antibiotics (e.g., broad-spectrum) → can raise INR via gut-flora or metabolic effects; many drug interactions exist.
- Alcohol → heavy/binge drinking increases bleeding risk and can alter INR; stick to low-risk guidance if permitted by your clinician.
- Illness, liver function, adherence, lab variability → each can shift INR and require closer monitoring.
Pro tips to keep INR steady
- Keep a simple weekly food template (greens portioned evenly across days).
- Always check drug interactions (including OTC and supplements) before starting.
- If your clinician supports it, consider home INR self-testing/monitoring in suitable cases.
- Re-test after significant changes (diet, antibiotics, illness, travel) per your clinic’s protocol.

FAQs
Do I have to avoid leafy greens on warfarin?
No. Aim for a consistent weekly intake rather than avoidance. Sudden changes (e.g., a “kale binge” after weeks of low Vit K) can swing INR.
Why: Vitamin K lowers INR; consistent intake helps stabilize results.
Can bananas or apples affect INR?
These fruits are low in vitamin K; typical amounts aren’t expected to meaningfully change INR again, consistency matters. (If you drink juices like cranberry or grapefruit, ask your clinician; some guidance advises avoiding them.)
Why is my INR all over the place even when I take my pills?
Common culprits: fluctuating vitamin K intake, new meds/antibiotics, variable alcohol, illness, or missed doses. Tighten consistency, review drug interactions with your clinician, and consider closer re-checks until stable.
Is INR < 1 even possible?
Yes. If a patient’s PT is shorter than the reference (or depending on reagent/ISI), INR can be < 1; it simply means clotting faster than the defined “normal.”
My INR is 3.5–4.0 what should I do?
That’s above typical 2.0–3.0 targets for many indications. Management is protocol-specific (dose hold/reduction, re-test timing), with more aggressive steps for higher INRs or bleeding. Call your clinician and follow local guidance.
What about mechanical valves are lower INRs ever okay?
For On-X aortic valves without thromboembolic risk factors, guidelines allow INR 1.5–2.0 after 3 months, with low-dose aspirin only under specialist direction. Other mechanical valves often target 2.5–3.5 depending on valve and position.
Can I drink alcohol on warfarin?
Many services allow light/moderate use; avoid binges and large day-to-day swings. Alcohol can increase bleeding risk and affect INR. Always confirm what’s safe for you.
Traveling while on warfarin any tips?
Keep diet and alcohol consistent, carry your dosing plan, know where/when you’ll test INR (portable/home testing is an option for selected patients), and list all meds.
Sources & further reading
- AHA, NHS, Mayo, university hospitals: Diet & vitamin K consistency (patient leaflets).
- NCBI Bookshelf: INR assessment & monitoring (formula, liver disease caveat).
- Practical-Haemostasis: ISI & INR explainer.
- Cleveland Clinic: PT/INR test patient info.
- ACC/AHA & Thrombosis Canada: Valve-specific INR targets (incl. On-X).
- AC Forum: High INR management and warfarin dosing practice materials.