Clinicians often search “hit calculator” when they mean the HIT (heparin-induced thrombocytopenia) 4Ts score a quick bedside tool to estimate pretest probability and guide testing and treatment. This article explains what HIT is, how the 4Ts score works, how to interpret it, and what to do next based on risk plus links straight to your calculator for fast use.
What is HIT, and why does the 4Ts score matters
HIT is an immune-mediated adverse reaction to heparin exposure in which antibodies against PF4–heparin complexes activate platelets, causing thrombocytopenia and a paradoxical pro-thrombotic state. Patients with HIT face a markedly increased risk of venous and arterial thrombosis, so early recognition and correct management are critical.
Because lab tests take time and can produce false positives, professional guidelines recommend using a clinical pretest score to drive testing decisions. The American Society of Hematology (ASH) explicitly recommends the 4Ts score rather than Gestalt to estimate the probability of HIT.

What is HIT, and why the 4Ts score matters
HIT is an immune-mediated adverse reaction to heparin exposure in which antibodies against PF4–heparin complexes activate platelets, causing thrombocytopenia and a paradoxical pro-thrombotic state. Patients with HIT face a markedly increased risk of venous and arterial thrombosis, so early recognition and correct management are critical.
Because lab tests take time and can produce false positives, professional guidelines recommend using a clinical pretest score to drive testing decisions. The American Society of Hematology (ASH) explicitly recommends the 4Ts score rather than Gestalt to estimate the probability of HIT.
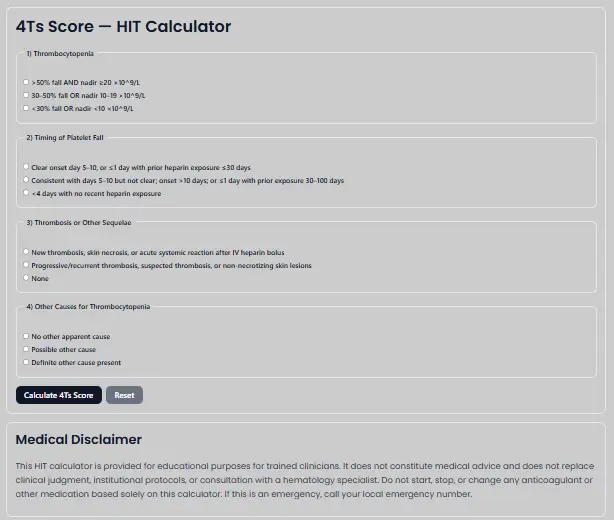
The 4Ts score, explained (0–8 points)
The 4Ts covers four domains Thrombocytopenia, Timing, Thrombosis (or other sequelae), and Other causes each scored 0, 1, or 2. Totals stratify risk:
- Low (0–3),
- Intermediate (4–5),
- High (6–8).
Below is a concise, guideline-aligned summary you can reference while using the calculator.
- Thrombocytopenia
2 => 50% fall and nadir ≥20×10⁹/L
1 = 30–50% fall or nadir 10–19×10⁹/L
0 = <30% fall or nadir <10×10⁹/L - Timing of platelet fall
2 = Clear onset days 5–14 after starting heparin (or ≤1 day with prior exposure ≤30d)
1 = Consistent with days 5–14 but not clear; or onset after day 14; or ≤1 day with prior exposure 30–100d
0 = ≤4 days without recent exposure - Thrombosis / other sequelae
2 = New thrombosis, skin necrosis, acute systemic reaction after IV heparin bolus, adrenal hemorrhage
1 = Progressive/recurrent thrombosis, suspected thrombosis, or non-necrotizing skin lesions
0 = None - Other causes of thrombocytopenia
2 = None apparent
1 = Possible
0 = Definite other cause present

How to interpret the 4Ts and act
Low (0–3): HIT is unlikely. Do not routinely order HIT lab tests; consider other causes of thrombocytopenia unless there’s significant uncertainty.
Intermediate (4–5) or High (6–8):
- Stop all heparin (including catheter flushes and LMWH).
- Start a non-heparin anticoagulant (see options below).
- Order a PF4/heparin immunoassay, and when available, confirm with a functional assay (e.g., SRA/HIPA) if the immunoassay is positive.
Testing strategy: immunoassay first, functional assay if positive
- Immunoassays (e.g., ELISA, poly- or IgG-specific) detect antibodies to PF4/heparin and are highly sensitive but less specific; higher optical density (OD) values correlate with a higher likelihood of true HIT. Rapid assays exist but vary in performance.
- Functional assays (e.g., SRA, HIPA) detect platelet-activating antibodies and are generally more specific, but availability is limited, and turnaround can be slow.
Guideline flow: With intermediate/high 4Ts, order an immunoassay; if positive and a functional assay is available, send the functional test. A functional test may be unnecessary when clinical probability is high and the ELISA is strongly positive.
Treatment: what to start, what to avoid
Immediate steps: Discontinue heparin and initiate a non-heparin anticoagulant. ASH suggests argatroban, bivalirudin, danaparoid, fondaparinux, or a DOAC; choose based on clinical context (hepatic/renal function, procedural needs, availability).
Intensity:
- Intermediate 4Ts with higher bleeding risk → consider prophylactic-intensity non-heparin anticoagulation.
- Intermediate 4Ts without high bleeding risk (or high 4Ts) → therapeutic-intensity non-heparin anticoagulation.
Warfarin: Avoid starting warfarin in acute HIT until platelets recover because of protein C depletion risk; transition later if needed per guideline-based durations. (See duration below.)
Platelet transfusion: Avoid routine transfusions in acute HIT unless there is active bleeding or a specific procedural need.
Duration of anticoagulation & imaging
- Acute HIT without thrombosis: Continue non-heparin anticoagulation at least until platelet count recovery (commonly ≥150×10⁹/L). Prolonged treatment beyond ~3 months is generally unnecessary unless thrombocytopenia or active HIT persists.
- HIT with thrombosis (HITT): Typical course 3–6 months of anticoagulation, assuming no other indication to extend.
- Screening for “silent” DVT: For acute HIT without clinically apparent thrombosis, ASH suggests bilateral leg ultrasonography; consider upper-extremity ultrasound if a central line is present.
Special situations (cardiac surgery, PCI, dialysis)
- Cardiac surgery / PCI: When feasible, delay surgery until HIT is remote; if urgent, bivalirudin is commonly suggested intra-procedurally (argatroban is an alternative where appropriate). Limit any heparin exposure to intraprocedural use only and avoid before/after.
- Renal replacement therapy: In acute HIT phases, ASH suggests argatroban, danaparoid, or bivalirudin for dialysis circuit anticoagulation; in certain recovered phases without other anticoagulation needs, regional citrate is suggested.
Evidence behind the 4Ts
The 4Ts score was originally proposed and validated in 2006 and subsequently validated across diverse settings. A large systematic review and meta-analysis (Cuker et al., 2012) showed the low 4Ts category has a very high negative predictive value, meaning most low-score patients do not have HIT. This is why guidelines emphasize 4Ts for initial triage instead of ordering tests for everyone with thrombocytopenia on heparin.
How to use our HIT (4Ts) Calculator effectively
- Gather key data first: baseline platelets, timing of heparin exposure, current platelet trend, thrombosis evidence (DVT/PE/arterial), skin findings, and alternative causes (sepsis, DIC, ITP, drugs).
- Enter the four T’s in the tool and compute.
- Follow the result:
- Low: Seek other causes; avoid routine HIT testing unless uncertainty is high.
- Intermediate/High: Stop heparin, start non-heparin anticoagulation, and order immunoassay ± functional assay as above.
FAQs
Can I rely on a low 4Ts score to rule out HIT?
A low 4Ts has high NPV in pooled analyses, so HIT is unlikely; reserve testing for unclear cases. Always re-evaluate if the clinical picture changes.
Which lab test should I order first?
With intermediate/high 4Ts, start with a PF4/heparin immunoassay; if positive and available, send a functional assay. Strongly positive ELISA results in a high-probability patient may suffice for management in settings lacking functional testing.
Which non-heparin anticoagulant should I choose?
ASH suggests argatroban, bivalirudin, danaparoid, fondaparinux, or a DOAC; tailor to organ function, procedural plans, and availability.
How long should I anticoagulate?
Without thrombosis, treat until platelet recovery (often to ≥150×10⁹/L) and generally avoid extending beyond ~3 months unless warranted. With thrombosis, the typical duration is 3–6 months.
Should I give platelets in HIT?
Routine platelet transfusions are discouraged in acute HIT unless the patient is bleeding or requires a procedure where transfusion is indicated.
Key sources
- ASH 2018 Guidelines on HIT (Blood Advances) and snapshot pages.
- ASH HIT Pocket Guide with the full 4Ts rubric, testing algorithm, and treatment suggestions.
- Systematic review/meta-analysis of 4Ts predictive value (Cuker et al., Blood 2012, open-access PMC).
- StatPearls (NCBI Bookshelf) overview of HIT pathophysiology and clinical features.
Medical disclaimer
This article and the HIT (4Ts) calculator are for educational use by trained clinicians. They do not replace clinical judgment, institutional protocols, or specialist consultation. In emergencies, follow local procedures immediately.