This guide shows you how to use a GRACE Calculator correctly in clinical work and exam settings. You will learn what the GRACE score means, which inputs to enter, how to interpret the outputs, and how to avoid the common pitfalls that lead to wrong numbers. The focus is acute coronary syndrome. The approach is practical. Steps are short and clear. The goal is safer decisions for house officers, registrars, intensivists, anesthetists, emergency teams, and students who round on real patients.
If you want to follow along with a working tool, open our calculator now: Try our free GRACE Calculator at the link below and keep it in view as you read:
What This Measurement Means In Medicine
The GRACE score is a validated risk tool for patients with acute coronary syndrome. It estimates the probability of death over admission to six months by combining clinical variables available at the bedside. The model was developed from a large international registry and later refined as GRACE version 2.0. It is widely used in emergency care, coronary care, and step down units to guide urgency of invasive evaluation and intensity of therapy.
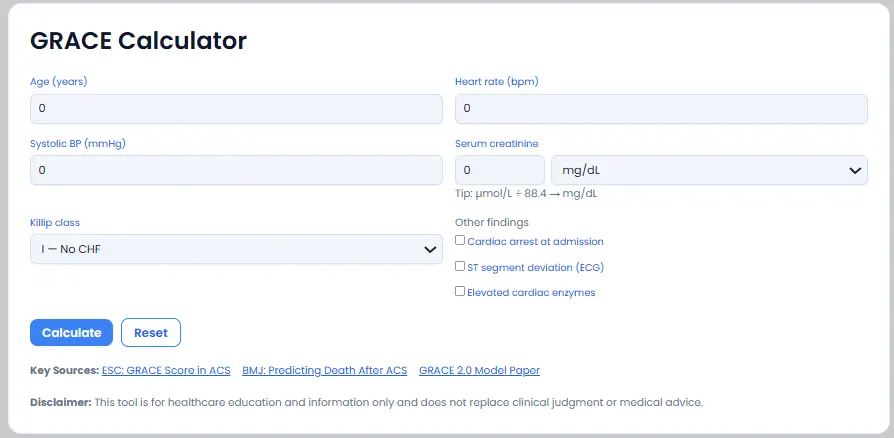
Inputs are age, heart rate, systolic blood pressure, serum creatinine, Killip class, presence of cardiac arrest at presentation, ST segment deviation on the electrocardiogram, and initial cardiac enzyme elevation. The calculator then outputs a points total and an estimated probability of death to six months.
Typical medical units are beats per minute for heart rate, millimeter of mercury for blood pressure, and either milligram per deciliter or micromole per liter for creatinine. Many hospitals chart creatinine in SI units. Converting correctly is essential because creatinine drives the risk estimate. The accepted relation is one milligram per deciliter equals eighty eight point four micromole per liter.
Two quick ways this calculator saves time:
- You have a patient with non ST elevation chest pain and raised troponin. Enter the variables and you can stratify risk in seconds. This supports early invasive planning when the score is high.
- During teaching rounds you can check expected risk ranges for two patients with different Killip class and blood pressure. That anchors the discussion around guideline style thresholds instead of guesswork.
Unit Conversions You Will Use Most
- One milligram per deciliter of creatinine equals about eighty eight point four micromole per liter. Use when labs report SI units but the calculator expects conventional units.
- One micromole per liter of creatinine equals about zero point zero one one three milligram per deciliter. Use when you have a creatinine in SI units and need a quick mental check of the number size.
- One millimeter of mercury equals about zero point one three three kilopascal. Use when notes or monitors show blood pressure in kilopascal and you want to confirm systolic inputs in millimeter of mercury.
How To Use The Calculator Correctly
Follow this workflow while your patient is being evaluated.
- Open the calculator
You will see fields for age, heart rate, systolic blood pressure, serum creatinine with unit choice, Killip class, and three check boxes for cardiac arrest, ST deviation, and enzyme elevation. - Choose the correct unit set
If creatinine is in micromole per liter, select the micromole option before typing the value. The tool converts to milligram per deciliter internally using the eighty eight point four factor. If your lab reports micromole per liter, you can also divide by eighty eight point four and type the converted milligram per deciliter. The embedded tip on the page matches this relation. - Enter values with appropriate significant figures
Age in whole years. Heart rate to the nearest whole beat per minute. Systolic blood pressure to the nearest whole millimeter of mercury. Serum creatinine to one or two decimals if you are entering milligram per deciliter, or a whole number if you are entering micromole per liter. This avoids artificial precision. - Select the Killip class
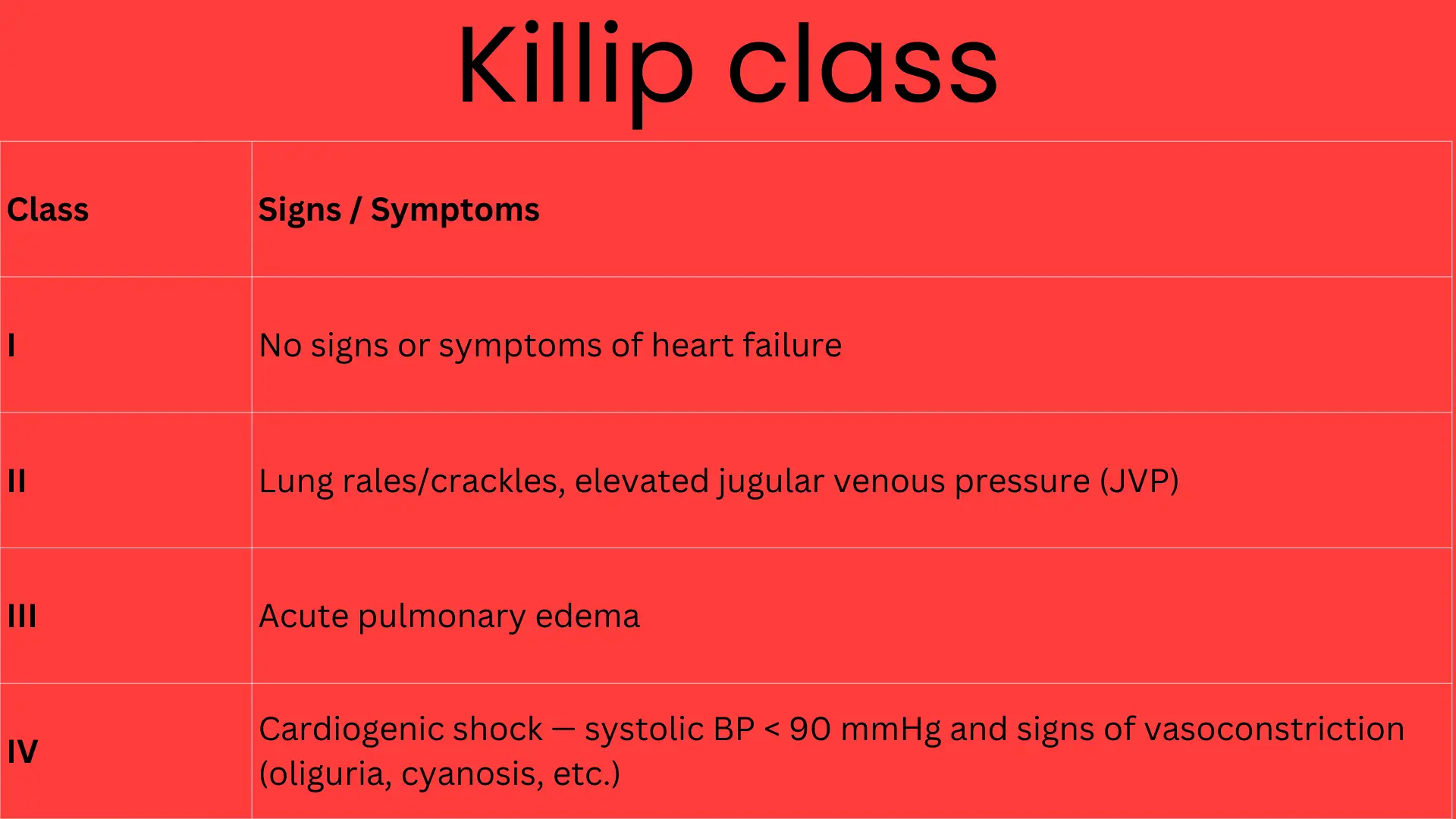
Choose I for no heart failure signs. Choose II for rales or raised jugular venous pressure. Choose III for pulmonary edema. Choose IV for cardiogenic shock. If unsure, review the exam and blood pressure again before selecting. Killip class is a powerful driver of risk. - Tick the other findings only if present at presentation
Cardiac arrest on arrival. ST segment deviation on initial electrocardiogram. Elevated cardiac enzymes at presentation. The model uses these variables as binary yes or no inputs in addition to the continuous ones. - Click Calculate
The result area shows the GRACE points and the estimated probability of death from admission to six months. This probability is based on the validated GRACE 2.0 logistic equation. - Cross check with a quick rule
Map the points to the common risk bands used in many studies. Low risk is about one to one hundred eight points. Intermediate risk is one hundred nine to one hundred forty. High risk is above one hundred forty. Many guidelines use a score above one hundred forty to trigger early invasive consideration in non ST elevation presentations. Your local policy may refine this. - Document the inputs and the output
Write age, heart rate, systolic blood pressure, creatinine with unit, Killip class, electrocardiogram change, enzyme status, GRACE points, and the probability percent. This allows any colleague to reproduce the result.
Mini Tutorials For Common Medical Tasks
Convert creatinine units before scoring
- Task. Your lab reports serum creatinine as one hundred ten micromole per liter. The calculator expects milligram per deciliter.
- Steps. Select micromole per liter in the unit drop down, type one one zero, then calculate. Or mentally divide one hundred ten by eighty eight point four which is about one point two four milligram per deciliter, then enter that value with the milligram per deciliter option.
- Why it matters. Wrong units can shift the risk band and change downstream decisions.
Rapid comparison of two patients on the ward
- Task. Patient A is seventy five with Killip I and normal blood pressure. Patient B is sixty two with Killip III and low systolic pressure.
- Steps. Enter both sets into the calculator one by one. Note the jump in points driven by Killip class and systolic pressure.
- Takeaway. The score helps anchor urgency of invasive evaluation when other features are borderline.
Interpret a result against thresholds
- Task. You calculated one hundred fifty two points in a patient with non ST elevation acute coronary syndrome.
- Steps. Check the band. Above one hundred forty indicates high risk. Use this to support early invasive strategy along with the clinical picture and high sensitivity troponin pathway.
- Reference. Several guideline summaries advise an early invasive approach in non ST elevation cases when the GRACE score is above one hundred forty.
Quick sanity check of the probability
- Task. Your output probability looks very high for a patient with good blood pressure and Killip I.
- Steps. Recheck units. Confirm that creatinine is not in micromole per liter while the calculator expects milligram per deciliter. Confirm that the ST deviation and enzyme boxes were not ticked by mistake. Recalculate.
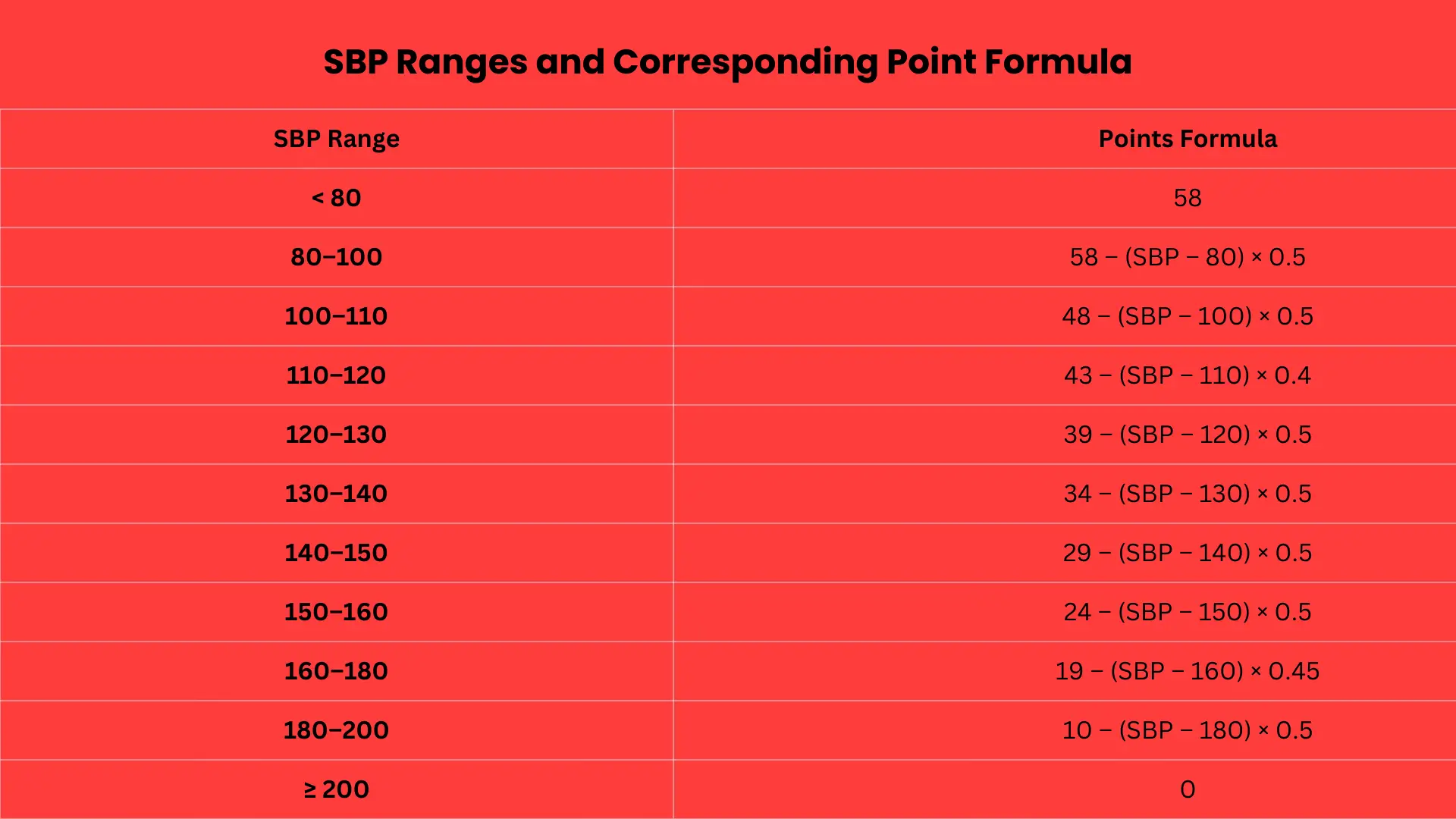
- Note. The GRACE 2.0 model is sensitive to creatinine, systolic blood pressure, and Killip class. Errors in these inputs change the curve a lot.
Common Mistakes And Fast Fixes
- Using micromole per liter in a milligram per deciliter field. Fix. Select the correct unit or divide by eighty eight point four before entry.
- Guessing Killip class. Fix. Re examine the patient for rales, jugular venous pressure, pulmonary edema, or shock and then select the right class.
- Rounding creatinine too early. Fix. Keep one or two decimals in milligram per deciliter or use whole numbers in micromole per liter.
- Forgetting to untick a box after testing a scenario. Fix. Use Reset before switching between cases.
- Interpreting any band as a diagnosis. Fix. Use the score to support risk aligned timing and therapy, not to label disease on its own.
Field Notes For Busy Clinicians
- Record the time of blood draw and electrocardiogram used for inputs. This keeps your number reproducible.
- When the score is close to a band edge, do not anchor. Combine with the troponin pathway and clinical stability.
- Killip class and systolic pressure drive large swings. Re assess these after initial treatment and recalc if the plan depends on the band.
- For teaching, compare the points change produced by a ten beat rise in heart rate or a twenty millimeter drop in systolic pressure. This builds intuition for trend effects.
- Document the full input set in the note so a colleague can confirm the result later without re entering unknowns.
FAQ
How to calculate GRACE score
Enter age, heart rate, systolic blood pressure, creatinine with the correct unit, Killip class, and tick the boxes for cardiac arrest, ST deviation, and enzyme elevation if present. Click Calculate to see the points and the percentage probability of death to six months. Use the one hundred forty cut point in non ST elevation presentations to frame urgency when supported by guidelines and the clinical picture.
What variables are included in the GRACE score
Age, heart rate, systolic blood pressure, serum creatinine, Killip class, cardiac arrest at admission, ST segment deviation, and initial cardiac enzyme elevation. These are the standard registry variables and form both the points and the logistic probability in GRACE 2.0.
What GRACE score is considered high risk
Many studies and summaries define high risk as a GRACE score above one hundred forty. This band often supports an early invasive approach in non ST elevation acute coronary syndrome when aligned with troponin based pathways and other high risk features.
How do I convert creatinine from micromole per liter to milligram per deciliter for the score
Divide the micromole per liter value by eighty eight point four. Example. One hundred ten micromole per liter becomes about one point two four milligram per deciliter. Select the correct unit in the calculator or type the converted value.
Does the GRACE score apply to both ST elevation and non ST elevation presentations
Yes. The score was developed across the spectrum of acute coronary syndrome. Clinical use differs by pathway. For non ST elevation presentations the score is commonly used to guide timing of invasive evaluation. For ST elevation presentations it is supportive but reperfusion decisions are not delayed for scoring.
How do I interpret the probability output
The percentage is the estimated probability of death from admission to six months based on the GRACE 2.0 model. Use it to communicate risk, to frame decisions about level of care, and to discuss benefits and burdens of invasive strategies. It does not replace clinical judgment.
Conclusion And Next Steps
You can now use a GRACE Calculator with confidence in emergency care and on the ward. You know the inputs, the units, and the risk bands. You can convert creatinine correctly, identify the Killip class, and read the output as a six-month probability. Next steps. Pick the correct unit for creatinine. Run two conversions to build speed. Save a quick table of band edges. Verify one output against the threshold rules used in your service.
Before your next case, open the tool and practice with two real numbers from your unit: