This guide explains how to use a FeNa calculator for real clinical work. You will learn which numbers to enter, what the output means, and how to avoid the most common traps when using FeNa in the setting of acute kidney injury. You will also learn when FeNa is not reliable and what to do in those cases.
By the end of this page, you will be able to collect the correct lab values, calculate FeNa in percent, interpret the value in terms of prerenal versus intrinsic renal causes of acute kidney injury, and document it safely. FeNa is often used in emergency and inpatient medicine to help decide if reduced kidney function is mainly due to low effective blood volume or due to tubular damage. FeNa is most useful in oliguric acute kidney injury in adults and becomes less reliable in patients with chronic kidney disease or in patients who recently received diuretics.
What this measurement means in medicine
FeNa stands for fractional excretion of sodium. It is the percentage of filtered sodium that actually leaves the body in the urine. A healthy kidney that is underperfused will try to hold on to sodium, so FeNa will be very low. A damaged kidney tubule cannot reabsorb sodium well, so FeNa goes up.
In practice, FeNa is used in patients with suspected acute kidney injury. A very low FeNa, usually under one percent, supports a prerenal picture. Prerenal means the kidney tissue itself is often structurally fine but the effective blood flow to it is low, such as in dehydration, heart failure with low forward flow, or cirrhosis with very low effective arterial volume. A higher FeNa, often above 2 percent, supports an intrinsic renal process, such as acute tubular necrosis, where the tubules are injured and lose sodium into the urine. Values in the middle are indeterminate and require more context.
Important caution. These cutoffs work best in oliguric adults, meaning low urine output, and when the patient is not on diuretics and does not have advanced chronic kidney disease. In chronic kidney disease, baseline tubular handling of sodium is altered, and the FeNa can appear falsely high even if the problem is still prerenal. In patients who have just received loop diuretics, sodium wasting is forced by the drug, so FeNa can appear high even if the kidney is under perfused.
Two short examples of how a calculator saves you time:
First, you do not need to do the full formula at the bedside. The tool accepts plasma sodium, plasma creatinine, urine sodium, and urine creatinine and returns FeNa with interpretation text, such as suggests prerenal or suggests intrinsic. This reduces arithmetic errors in a stressed moment.
Second, FeNa supports communication. Instead of saying kidneys maybe dry, you can say FeNa is zero point six percent with oliguria which supports a prerenal picture, will start volume guided resuscitation. This is clearer for handoff and for notes.
Unit conversions you will use most
All inputs in the FeNa calculator are concentration values, not pressures. You will mainly deal with sodium and creatinine in plasma and urine. The calculator already handles common unit differences.
One milligram per deciliter creatinine equals about eighty eight point four micromole per liter. This conversion matters because many labs outside the United States report creatinine in micromole per liter. The calculator code you provided converts micromole per liter back to milligram per deciliter internally before calculating FeNa.
For sodium, millimole per liter and milliequivalent per liter are numerically the same because sodium is a single charge cation. The calculator treats mEq per liter and mmol per liter as equivalent for sodium. That means you can safely enter either one as long as you choose the right unit from the dropdown.
Pressure based conversions like millimeter of mercury to kilopascal or pound per square inch are not directly needed for FeNa. Those conversions are more relevant to ventilator pressure, vascular pressure, and gas systems. They do not enter the fractional excretion calculation, which is purely chemistry based. I will still state two examples for completeness because they come up in the same critical care setting:
One millimeter of mercury equals about zero point one three three kilopascal. Use this if you are reading an arterial line waveform in kilopascal and need millimeters of mercury for charting.
One pound per square inch equals about six thousand eight hundred ninety four point seven six pascal. Use this when reading oxygen cylinder or device specs in engineering units, for example when moving a critically ill patient with acute kidney injury and shock who is also on oxygen support.
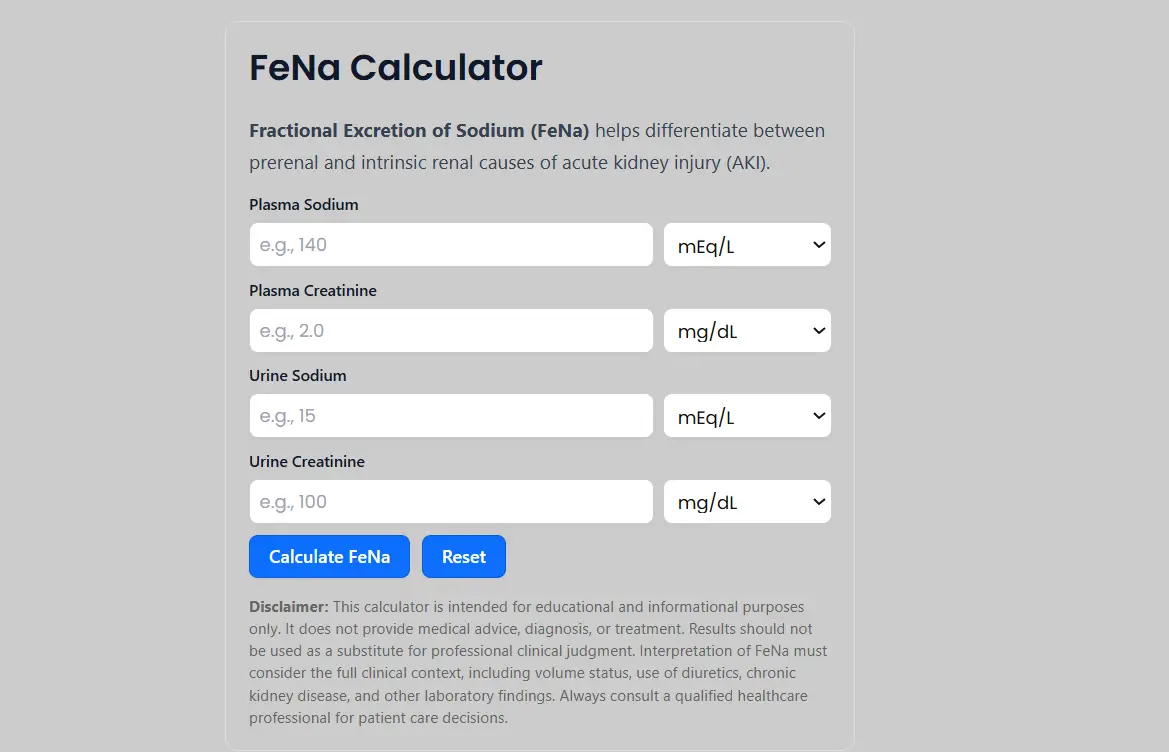
How to use the calculator correctly
The FeNa calculator includes four fields and gives you a percentage result with an interpretation line.
Follow this numbered workflow:
- Get paired labs. You need plasma sodium, plasma creatinine, urine sodium, and urine creatinine drawn at roughly the same clinical time. Ideally within about two hours of each other. This is important because FeNa assumes these values reflect the same physiologic state.
- In the calculator, enter plasma sodium. Choose mEq per liter or mmol per liter from the unit menu. For sodium those are equivalent.
- Enter plasma creatinine. Choose milligram per deciliter or micromole per liter. The tool converts micromole per liter to milligram per deciliter for you using one milligram per deciliter equals eighty eight point four micromole per liter.
- Enter urine sodium with the correct unit. Low urine sodium is common in prerenal states because the kidney is conserving sodium.
- Enter urine creatinine with the correct unit. Higher urine creatinine reflects more concentrated urine, which often appears in prerenal states because the kidney is trying to hold on to water and sodium.
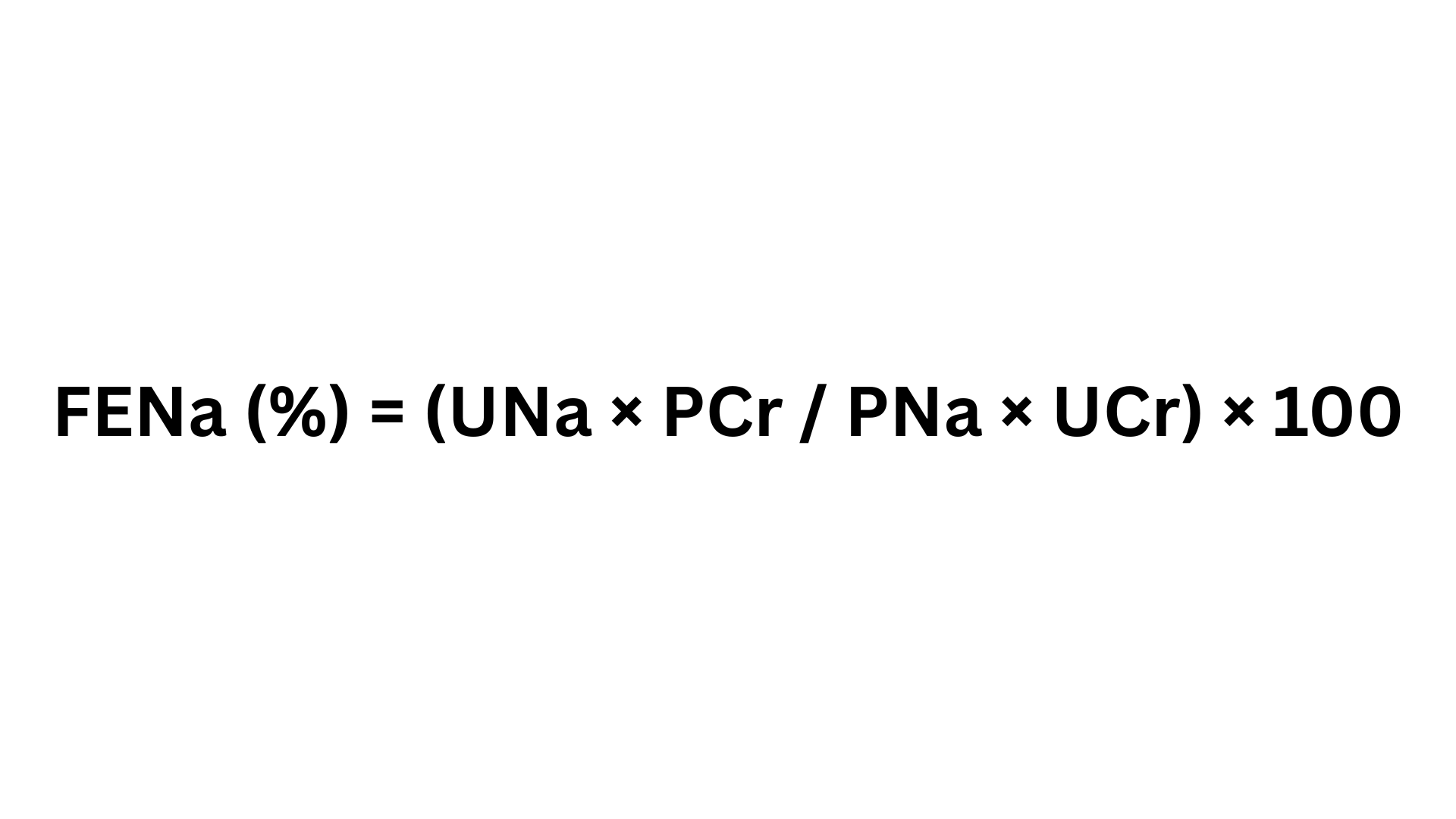
- Click Calculate FeNa. The calculator applies the standard formula: FeNa percent equals one hundred times urine sodium times plasma creatinine divided by plasma sodium times urine creatinine. Written another way:
FeNa percent equals one hundred multiplied by open bracket urine sodium multiplied by plasma creatinine close bracket divided by open bracket plasma sodium multiplied by urine creatinine close bracket. - Read the FeNa percent shown on screen. The calculator then gives a short note such as suggests prerenal cause of acute kidney injury if less than one percent or suggests intrinsic renal cause if above two percent. This mirrors the classic interpretation.
- Add clinical checks. Confirm the patient is oliguric. Ask if they recently received a loop diuretic. Ask if they already have advanced chronic kidney disease. These factors can break the usual cutoffs.
Our fena calculator already does two good safety things. It allows you to choose units in micromole per liter and in milligram per deciliter for creatinine, and it warns about diuretics and chronic kidney disease in the note under the result. Keeping that visible on screen is important for honest use.
Mini tutorials for common medical tasks
FeNa in suspected prerenal acute kidney injury
Clinical picture
A patient in the emergency department is hypotensive and oliguric. You suspect prerenal acute kidney injury from volume depletion.
Steps
Get plasma sodium, plasma creatinine, urine sodium, and urine creatinine from samples taken at about the same time. Enter those values into the FeNa calculator. Click Calculate FeNa.
If FeNa is less than one percent and urine output is low, this supports a prerenal pattern. In a prerenal pattern, the kidney is trying to hold sodium and water to protect perfusion. You can document FeNa zero point six percent with oliguria, supports prerenal pattern, starting cautious fluid resuscitation.
Important. You are not done. You must still confirm clinically. Low FeNa in isolation is not a diagnosis. It is a clue.
FeNa in suspected intrinsic acute kidney injury
Clinical picture
A patient in the intensive care unit after septic shock has rising creatinine and muddy brown casts on urine microscopy.
Steps
Again, collect paired plasma and urine sodium and creatinine. Enter into the calculator.
If FeNa is above two percent, that supports an intrinsic renal pattern such as acute tubular necrosis. Tubules are injured and cannot reabsorb sodium. You can write FeNa three point two percent with granular casts, supports intrinsic tubular injury pattern in septic acute kidney injury.
Note that some patients with intrinsic renal injury still show FeNa below one percent, such as in early sepsis, contrast associated injury, or hepatorenal physiology. That is why FeNa must be interpreted with the whole picture.
When to consider FEUrea instead
If the patient recently received a loop diuretic, FeNa may appear higher because the drug forces sodium loss in urine. In that setting, many clinicians calculate fractional excretion of urea instead. A FEUrea under about thirty five percent is often used to suggest a prerenal state even when diuretics are in play, although even FEUrea is not perfect and recent studies question how superior it really is.
Trend rather than snapshot
Repeat FeNa during ongoing shock resuscitation is usually not needed. Instead you should trend creatinine, urine output, and clinical perfusion. FeNa is mainly a classification tool early in the workup, not a management target you try to normalize.
Common mistakes and fast fixes
Using values that were not drawn at the same time. Fix: use plasma and urine electrolytes that are collected as a pair, ideally within about two hours.
Assuming FeNa below one percent automatically means prerenal. Fix: check for situations where intrinsic injury can also have very low FeNa such as contrast injury, hepatorenal physiology, or early sepsis.
Interpreting FeNa in a patient on loop diuretics without caution. Fix: consider FEUrea or clinical examination instead, because diuretics can falsely raise FeNa.
Ignoring chronic kidney disease. Fix: in chronic kidney disease the tubular handling of sodium is already altered, so FeNa can be higher even if the trigger is still prerenal. Document the baseline kidney status.
Using FeNa in non oliguric patients as if it has the same meaning. Fix: FeNa was mainly validated in oliguric acute kidney injury. In non oliguric states the interpretation is weaker.
Field notes for busy clinicians
Always write urine output status with the FeNa result. FeNa without urine output is incomplete.
Document recent diuretic exposure in the same line as the FeNa result. This prevents misinterpretation on rounds.
Do not chase the number. Use FeNa to frame prerenal versus intrinsic suspicion, then confirm with physical exam, point of care ultrasound for volume status, lactate or sepsis workup, and urine sediment.
Remember that FeNa is a tool, not a verdict. It can support you, but it cannot replace bedside judgment.
Save the link to the FeNa calculator in your admission note template so juniors can calculate quickly and record their assumptions. You can point them to FeNa calculator as the working tool.
FAQ
How to calculate FeNa
Use this formula. FeNa percent equals one hundred times urine sodium times plasma creatinine divided by plasma sodium times urine creatinine. Enter plasma sodium, plasma creatinine, urine sodium, and urine creatinine into the calculator and click Calculate FeNa. The tool returns the FeNa in percent and a short interpretation line.
What FeNa cutoff suggests a prerenal cause
Classically, FeNa less than one percent in an oliguric adult suggests a prerenal state with low effective kidney perfusion. Examples include dehydration, low output heart failure, or advanced cirrhosis. This rule is weaker if the patient recently received diuretics or already has chronic kidney disease.
What FeNa cutoff suggests intrinsic acute tubular injury
Many clinicians use FeNa above two percent to suggest intrinsic tubular damage such as acute tubular necrosis, especially in septic shock or ischemic injury. Values in the middle, such as one to two percent, are indeterminate and must be interpreted in context.
Is FeNa reliable if the patient received diuretics
Diuretics increase urinary sodium excretion, which can raise FeNa even if the problem is still prerenal. In that setting, many teams prefer fractional excretion of urea and bedside assessment of perfusion. Even FEUrea is not perfect, but it tends to be less affected by loop diuretics.
Does FeNa work in chronic kidney disease
FeNa is less reliable in chronic kidney disease because damaged kidneys cannot reabsorb sodium normally, so FeNa may be higher even in prerenal states. You should document baseline kidney function and interpret with caution.
Do I still need urine microscopy if I have FeNa
Yes. Muddy brown granular casts still matter for intrinsic tubular injury such as acute tubular necrosis. FeNa is a support tool, not a replacement for clinical examination and urine sediment review.
Can I just look at urine sodium instead of calculating FeNa
No. Urine sodium alone can be misleading because it depends on water handling and concentration. FeNa compares urine sodium to plasma sodium and at the same time corrects for concentration using creatinine in both fluids. That is why you must enter both sodium and creatinine from urine and from plasma.
Where can I calculate FeNa quickly
Use the live tool here: FeNa calculator. It accepts common units, converts creatinine automatically, and gives an interpretation line that mentions prerenal and intrinsic patterns.
Conclusion and next steps
You can now use a FeNa calculator correctly and safely. You know which labs to collect. You know how to enter sodium and creatinine values with the right units. You know how to read the percent output and link it to prerenal or intrinsic patterns in acute kidney injury. You also know the limits. Diuretics, chronic kidney disease, and non oliguric states reduce accuracy.
Your next steps are simple.
Take paired plasma and urine labs.
Run the FeNa once using the calculator.
Write the value, the urine output status, and any diuretic exposure in your note.
If the story is unclear, consider FEUrea, urine sediment, and bedside assessment of volume.