This article explains how to use an anion gap calculator accurately and confidently across clinical settings, including medical study, ward rounds, emergency care, anesthesia, respiratory therapy, and public health practice. During the early days of my house job, I found anion gap calculations confusing. I was not aware that two different formulas exist, when potassium should be included, or how to calculate and interpret the anion gap quickly under clinical pressure. That gap in understanding is common among junior doctors and students.
This guide breaks the process down clearly by showing which values to enter into an anion gap calculator, how to interpret the output correctly, when albumin correction should be considered, and how to avoid frequent calculation and unit errors. Only essential worked steps are included, so the focus stays on clinical reasoning rather than unnecessary math, helping you use the anion gap calculator efficiently and safely in real practice.
By the end you will know how to choose the right inputs, run a fast sense check, and document a safe interpretation for medical students and medical professionals. You will also know when a correction is useful and when it may not change your action.
What this measurement means in medicine
The anion gap is a value derived from routine chemistry results. It reflects the difference between the main measured cations and the main measured anions in plasma. In practice we compute sodium minus the sum of chloride and bicarbonate. Potassium may be added in some laboratories, but most clinical use excludes potassium. The gap rises when unmeasured anions accumulate. The gap can be low when albumin is very low or when unmeasured cations are present.
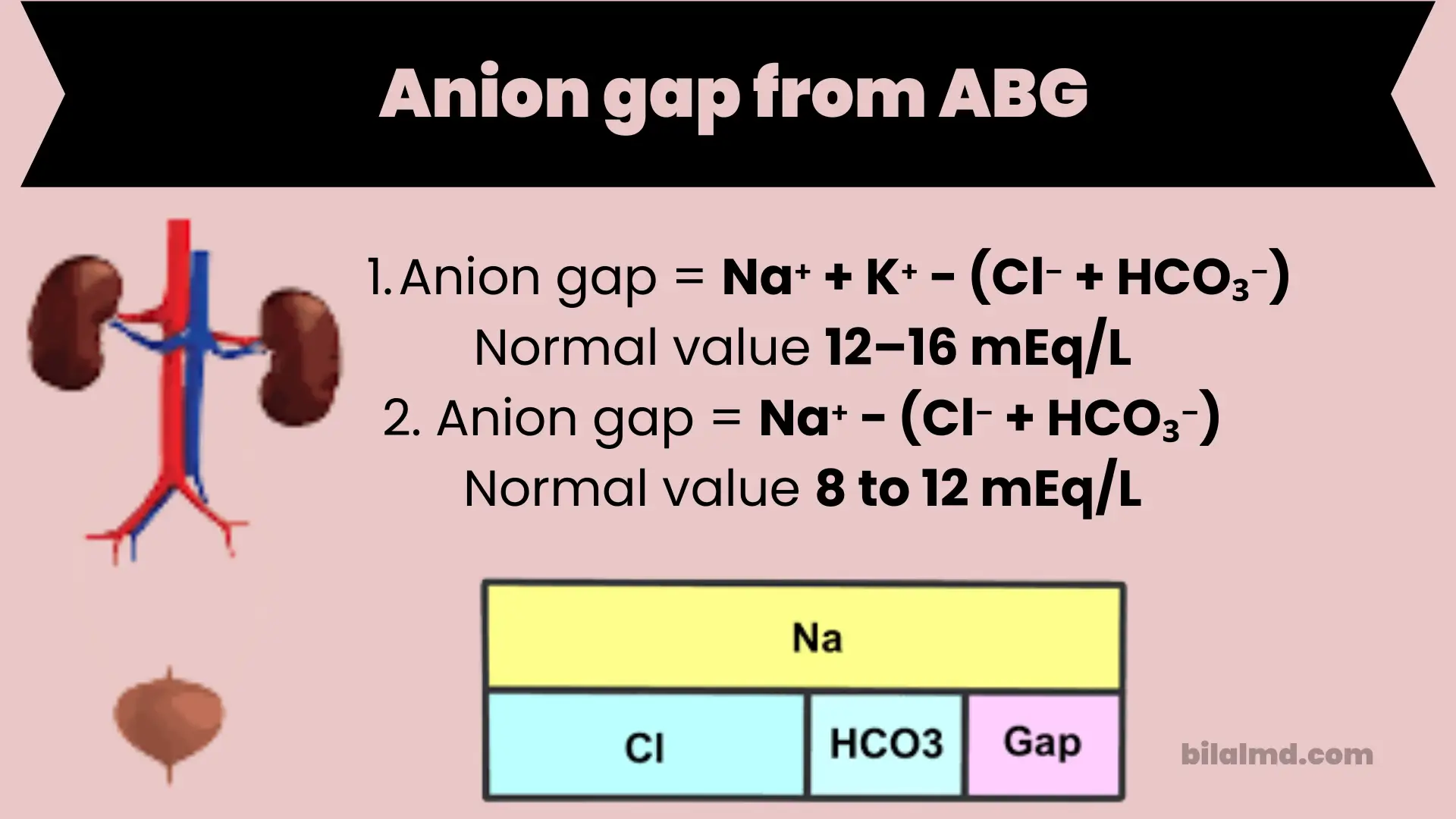
There is no single universal normal range. Each laboratory sets its own reference interval based on its method. Many sources cite about eight to twelve millimoles per liter when potassium is not included. Always use the range printed with your patient results.
Two short examples of time saved
First, you can turn three numbers into one figure that helps screen for a high gap metabolic acidosis and focus the differential. Second, you can trend the gap during treatment of conditions such as ketoacidosis or lactic acidosis to see if the unmeasured anion load is resolving.
Unit conversions you will use most
Millimoles per liter and milliequivalents per liter are numerically equal for sodium, chloride, and bicarbonate because each carries a single charge. Use this when a lab or paper switches between these unit labels.
Bicarbonate on a chemistry panel and HCO₃⁻ on a blood gas can differ slightly due to the method. Use the chemistry bicarbonate for a stable baseline when both are available. Use one source consistently during trending.
If your team reads devices that present pressure units during respiratory discussions, remember that these do not enter the anion gap calculation. They appear here only for cross discipline awareness. You can ignore pressure conversions for the gap, since all inputs are in millimoles per liter.
How to use the calculator correctly
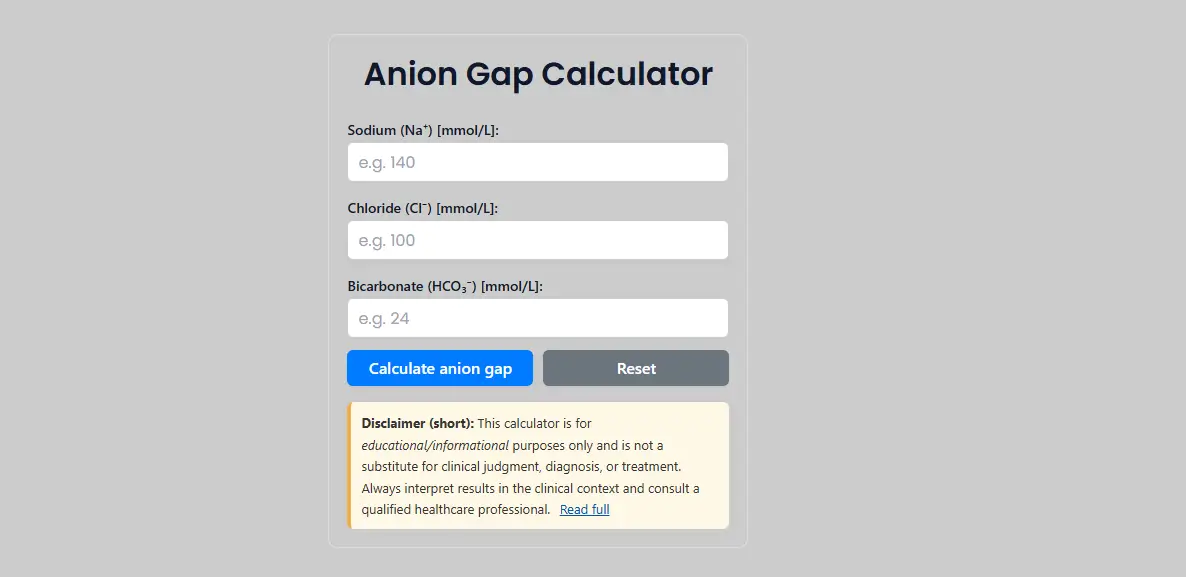
Follow this numbered workflow on the BilalMD page.
- Enter sodium in millimoles per liter. Use the value on the current chemistry report.
- Enter chloride in millimoles per liter. Confirm the same sample time if possible.
- Enter bicarbonate in millimoles per liter. Use the chemistry bicarbonate when available for consistency.
- Click Calculate anion gap. The result shows the gap in millimoles per liter. The basic formula is sodium minus chloride plus bicarbonate.
- If albumin is low, consider a corrected anion gap. A common method adds about two point five times the difference between four and the albumin in grams per deciliter. For example if albumin is two point zero, the adjustment is about five. Add this to the measured gap to estimate a corrected value. See your local guidance because formulas and cutoffs vary.
- Read the output with your laboratory reference interval. There is no single normal for all labs. A value above the lab upper limit suggests extra unmeasured anions and supports a high gap acidosis context. A value inside the lab range with acidosis suggests a normal gap pattern, often with higher chloride.
- Do a quick mental check. Sodium one hundred forty, chloride one hundred, bicarbonate twenty four gives anion gap sixteen. Your mental subtraction should match the screen.
- Document the number and the context rather than a diagnosis. State whether albumin was low and whether you corrected. Note the likely drivers you are investigating, such as lactate or ketones, without overclaiming.

Guidance on three details
Choosing the correct unit set. Use millimoles per liter throughout. If a report shows milliequivalents per liter for these ions, the numbers are the same in practice.
Significant figures. Whole numbers are fine. Use one decimal place only if your lab reports one. Rounding beyond the lab display adds noise.
Gauge versus absolute. This distinction applies to pressure devices and does not affect the anion gap, which uses concentration values.
Mini tutorials for common medical tasks
Compute a basic anion gap and write a safe note
Numbers
Sodium one hundred forty
Chloride one hundred
Bicarbonate twenty four
Steps
Enter the three values. Click Calculate. The result is sixteen millimoles per liter. In your note write anion gap sixteen using lab chemistry values. No albumin correction applied. Screen supports the presence of unmeasured anions. Plan to check lactate and ketones.
Correct for low albumin when appropriate
Numbers
Anion gap twelve
Albumin two point zero grams per deciliter
Steps
Compute correction. Four minus two equals two. Two times two point five equals five. Corrected gap equals twelve plus five equals seventeen. In your note write corrected for low albumin using Figge style adjustment. Use your local cutoffs to interpret.
Use the gap to focus a differential without diagnosing
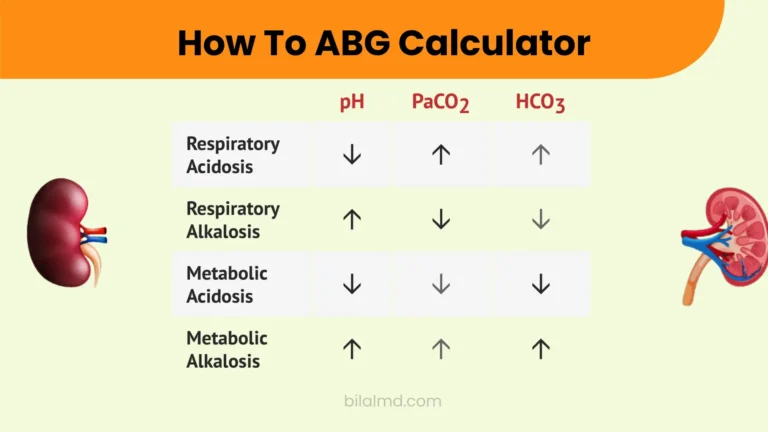
A high gap pattern suggests an increased load of unmeasured anions such as lactate or ketoacids or toxins in the right context. A normal gap pattern with acidosis often points toward chloride gain or bicarbonate loss from the gut or kidney. The calculator supports pattern recognition. The clinical picture and tests confirm the cause.
Quick trending during treatment
Recheck sodium, chloride, and bicarbonate as therapy proceeds. Enter new values and compare with the prior gap. A falling gap suggests that the unmeasured anion burden is shrinking. Pair this with pH, bicarbonate, and clinical status for decisions.
Common mistakes and fast fixes
Using a chemistry bicarbonate from a different time than the sodium and chloride. Fix by using values from the same draw when possible.
Switching between blood gas and chemistry bicarbonate during trending. Fix by choosing one source and staying with it for a case series.
Forgetting to consider albumin in very low albumin states. Fix by noting albumin and considering a correction when albumin is far below normal.
Treating the gap as a diagnosis. Fix by using the number to structure a differential and then ordering targeted tests such as lactate or beta hydroxybutyrate.
Over interpreting a low gap without checking for error or paraprotein. Fix by confirming the lab method and considering albumin, lithium, bromide interference, or paraproteinemia when the clinical picture fits.
Field notes for busy clinicians
Write the raw gap and whether you corrected for albumin so others can follow your logic.
If the gap and the clinical picture disagree, repeat the chemistry and check for sampling or reporting issues before you chase rare causes.
When acidosis is present but the gap is normal, think chloride gain or bicarbonate loss. Then use urine studies or clinical context to narrow further.
Trend the gap, the bicarbonate, and the pH together. A single value rarely decides care.
Bookmark your laboratory reference interval for fast reference. There is no single normal that applies to every analyzer.
FAQ
How do I calculate the anion gap
Use sodium minus the sum of chloride and bicarbonate. Example. One hundred forty minus one hundred plus twenty four equals sixteen millimoles per liter. The calculator performs this automatically once you enter the three values.
How is the anion gap calculated when potassium is included
Some formulas include potassium. In that case use sodium plus potassium minus chloride plus bicarbonate. Many clinical pathways exclude potassium, and reference ranges differ based on the formula used. Check your lab notes.
How do I calculate a corrected anion gap for low albumin
A common bedside rule is corrected gap equals measured gap plus two point five times four minus albumin in grams per deciliter. Use local guidance for your cutoff values and remember that not all experts agree that correction changes actions in every case.
What is a normal anion gap
There is no single normal. Many sources cite about eight to twelve millimoles per liter when potassium is not included. Your laboratory provides the interval that fits its method and analyzer. Always read the range printed with the patient report.
What does a low anion gap mean
Low values are uncommon. They can occur with very low albumin or with increases in unmeasured cations. They can also reflect laboratory method issues. Recheck the sample and review the clinical picture before you assign a cause.
What does a high anion gap suggest
It supports the presence of extra unmeasured anions. Common examples include lactate in tissue hypoxia and ketoacids in diabetic ketoacidosis. Use the number to focus testing rather than to label a diagnosis.
Is the anion gap the same as the urine anion gap
No. The usual bedside anion gap refers to serum. A urine anion gap exists but serves a different purpose and has wide variability. Do not mix the two in one note.
Can I rely on my pulse oximeter to help with the anion gap
No. Pulse oximeters report saturation and pulse rate. They do not provide sodium, chloride, or bicarbonate. Use a chemistry panel to compute the gap.
Conclusion and next steps
You can now use an anion gap calculator with confidence. Pick the correct unit. Enter sodium, chloride, and bicarbonate from the same draw. Consider an albumin correction in very low albumin states using your local rule. Read the result against your laboratory reference interval. Verify one output with a mental subtraction, and document the value with context rather than a diagnosis. For practice, run two sample cases, save the albumin correction constant you use most, and verify one output against a quick rule before you act.