This article teaches you how to use an ABG calculator to interpret arterial blood gas results with confidence. You will learn which inputs to enter, how to read the outputs, how to convert common units, and how to avoid the errors that lead to wrong conclusions. The goal is safe and repeatable interpretation for study, ward practice, critical care, anesthesia, respiratory therapy, and public health.
By the end, you will be able to pick the correct unit set, analyze pH, PaCO₂, and bicarbonate in a logical order, check expected compensation with a quick rule, and write a short interpretation that guides care without overclaiming. These habits match widely used instructional steps for ABG analysis.
What this measurement means in medicine
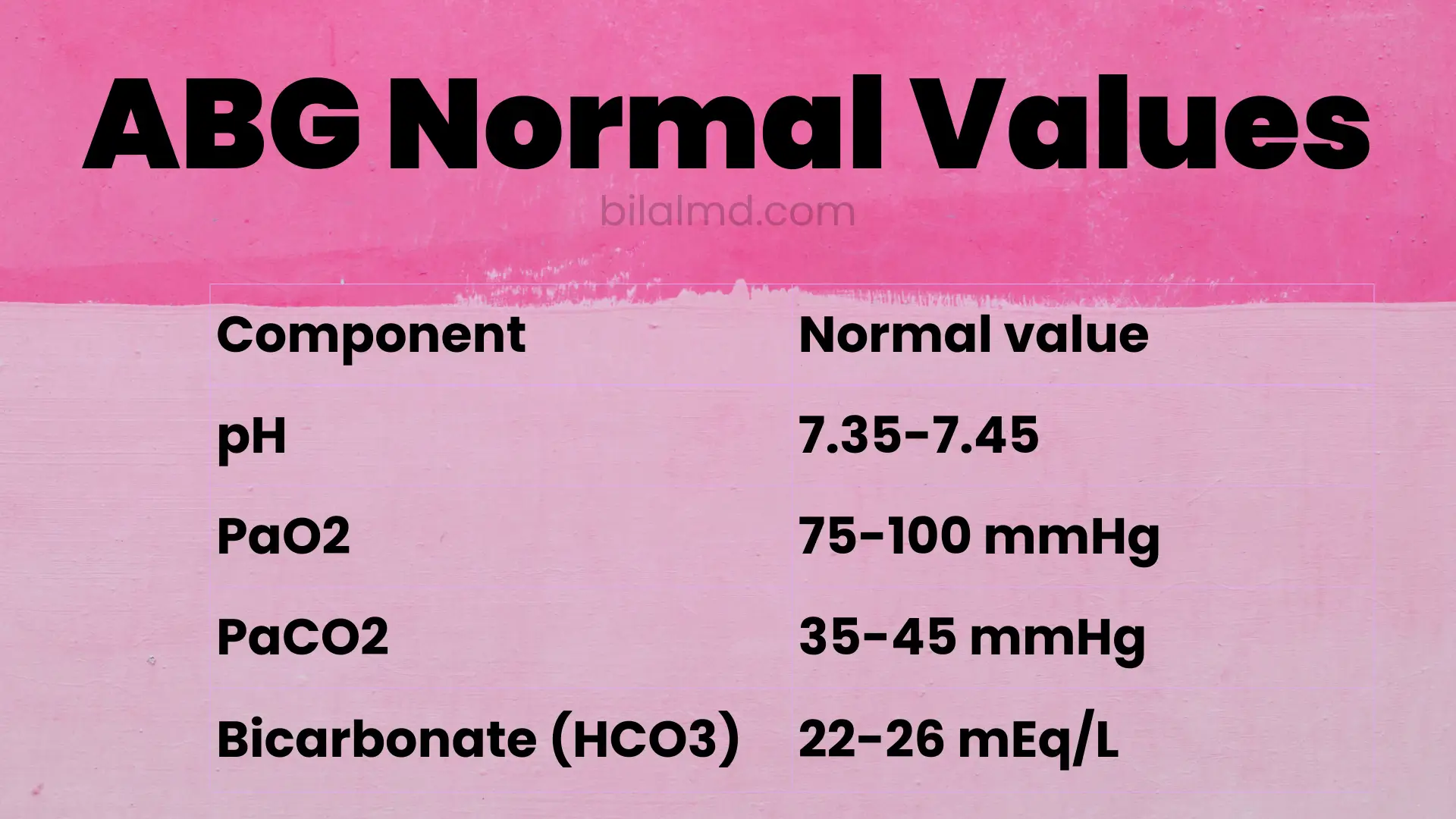
An ABG reports the acidity of blood and key dissolved gases. pH shows acidity. PaCO₂ shows the respiratory component. Bicarbonate shows the metabolic component. You can think of pH as the headline and PaCO₂ and bicarbonate as the two levers that move it. Values outside the usual adult ranges suggest acidosis or alkalosis with a respiratory or metabolic driver. Typical adult reference ranges are
- pH 7.35 to 7.45
- PaCO₂ 35 to 45 millimeters of mercury
- bicarbonate 22 to 26 milliequivalents per liter.
Two ways a calculator saves time. First, it keeps all three inputs on one screen and formats the interpretation so you see the likely primary disorder at a glance. Second, it lets you switch between millimeters of mercury and kilopascal for PaCO₂ with correct conversion, which prevents unit errors during teaching rounds and simulation practice.

Unit conversions you will use most
One millimeter of mercury equals about zero point one three three kilopascal. Use this when a report lists PaCO₂ in kilopascal and you prefer millimeters of mercury for charting.
One kilopascal equals about seven point five zero zero six two millimeters of mercury. Use this when your calculator gives PaCO₂ in kilopascal and the ventilator note is in millimeters of mercury.
For bicarbonate, milliequivalents per liter and millimoles per liter are numerically the same in practice. This is because bicarbonate carries a single charge. Use either label as shown by your lab.
The water column and engineering pressure relations are less central to ABG interpretation but may appear in ventilator and gas supply work. One pound per square inch equals about six thousand eight hundred ninety four point seven six pascal. Use this for equipment specifications and oxygen systems.
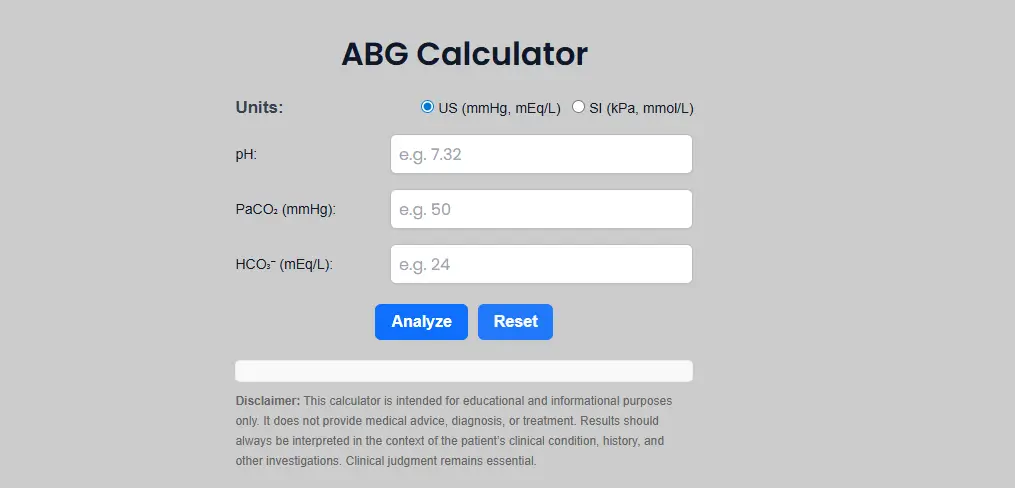
How to use the calculator correctly
Follow this numbered workflow each time. Keep entries in the units shown on the form.
- Set units. Choose US units for PaCO₂ in millimeters of mercury and bicarbonate in milliequivalents per liter. Choose SI units for PaCO₂ in kilopascal and bicarbonate in millimoles per liter. The calculator can convert PaCO₂ between systems.
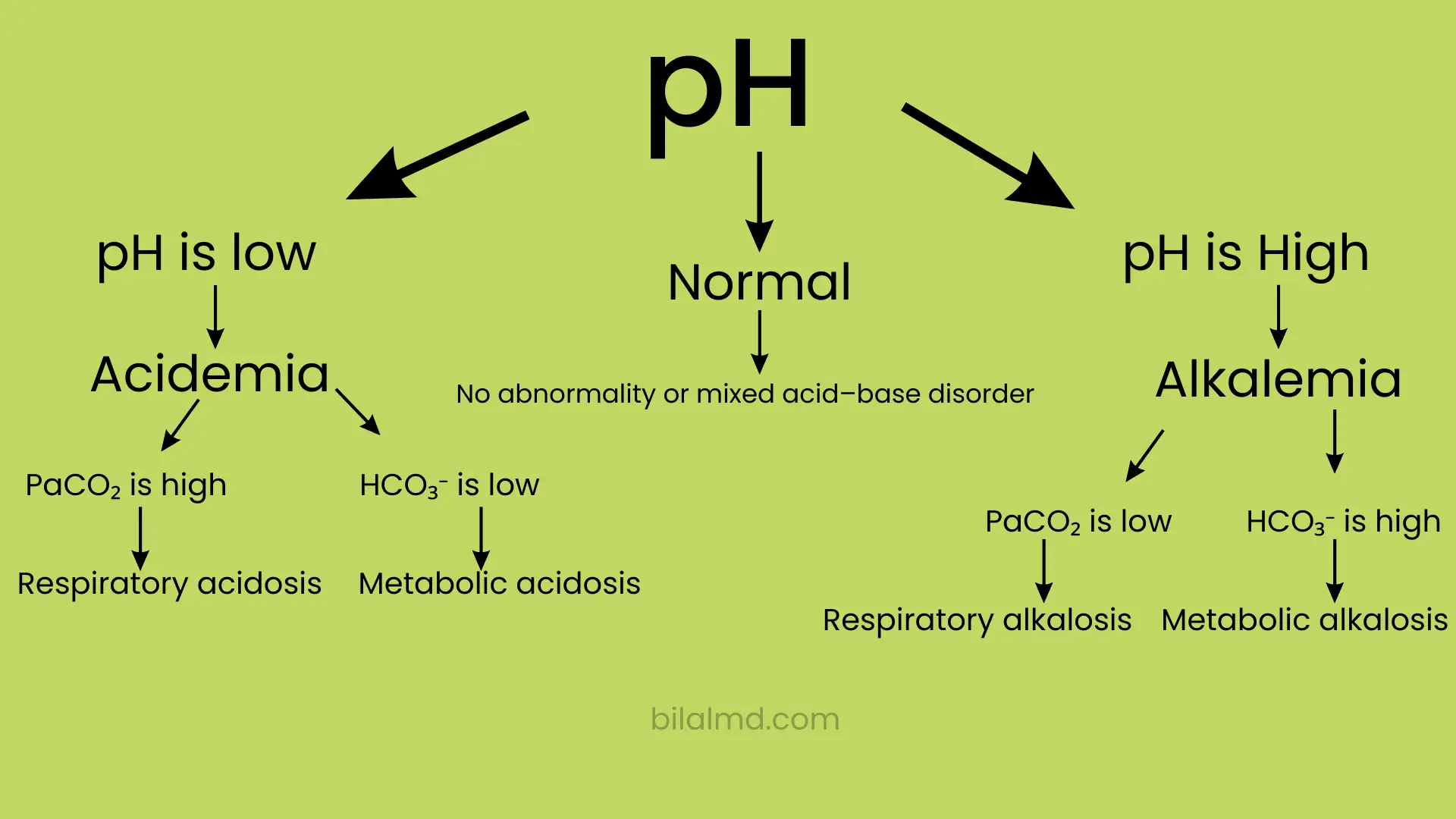
- Enter pH. Use two decimals if available. pH below 7.35 indicates acidemia. pH above 7.45 indicates alkalemia. If pH is inside the range, compensation or mixed disorders may be present.
- Enter PaCO₂. This is the respiratory variable. Higher PaCO₂ pushes pH down. Lower PaCO₂ pushes pH up. Check the unit label before you type.
- Enter bicarbonate. This is the metabolic variable. Lower bicarbonate pushes pH down. Higher bicarbonate pushes pH up. Use the chemistry value if both chemistry and blood gas bicarbonate are available and you want a stable baseline for trending.
- Read the primary process. The calculator will classify patterns such as respiratory acidosis or metabolic alkalosis and will display the values you typed with normal ranges for quick context.
- Cross check expected compensation when needed. In a pure metabolic acidosis, expected PaCO₂ equals one point five times bicarbonate plus eight, with a tolerance of plus or minus two. If measured PaCO₂ is higher than expected, there is a superimposed respiratory acidosis. If lower than expected, there is a superimposed respiratory alkalosis. This fast check helps reveal mixed disorders.
- Record your interpretation. Use a single line that names the primary disorder and any compensation or mix. Example. Primary metabolic acidosis with appropriate respiratory compensation. Add clinical data and plan rather than a diagnosis label alone.
Guidance on three details
Choosing the correct unit set. Match the unit family to the device and to your local documentation standard. Use the conversion factors above when switching between kilopascal and millimeters of mercury.
Significant figures. Two decimal places for pH and one decimal place for PaCO₂ and bicarbonate are usually adequate. Extra digits do not improve clinical decisions.
Gauge versus absolute. This distinction applies mainly to pressure devices and gas supply engineering. It does not change how you enter PaCO₂ in the calculator, since the analyzer reports a calibrated partial pressure value for clinical use.
Mini tutorials for common medical tasks
Rapid interpretation of a classic pattern
Case. pH 7.28, PaCO₂ 28 millimeters of mercury, bicarbonate 13 milliequivalents per liter.
Steps. Enter the values. The pH shows acidemia. Bicarbonate is low. This points to metabolic acidosis. Use the compensation check. Expected PaCO₂ equals one point five times thirteen plus eight which is about twenty seven point five plus or minus two. Measured PaCO₂ is twenty eight which is appropriate compensation. Write. Primary metabolic acidosis with appropriate respiratory response. Consider lactate or ketones.
Convert PaCO₂ between kilopascal and millimeters of mercury
You have PaCO₂ of five point three kilopascal on a blood gas report. You want millimeters of mercury for rounds. Multiply by seven point five zero zero six two. Five point three becomes about thirty nine point eight millimeters of mercury which sits inside the adult normal range.
Distinguish respiratory from metabolic in a near normal pH
Case. pH 7.40, PaCO₂ 51 millimeters of mercury, bicarbonate 30 milliequivalents per liter.
Steps. A normal pH does not rule out a disorder. With higher PaCO₂ and higher bicarbonate, the pattern is respiratory acidosis with metabolic compensation. This appears in chronic hypercapnia. Document the mix and trend against prior values.
Use normal ranges and a clean sentence in your note
Normal adult ranges are pH 7.35 to 7.45, PaCO₂ 35 to 45 millimeters of mercury, and bicarbonate 22 to 26 milliequivalents per liter. A clean note example. ABG shows pH 7.33, PaCO₂ 55, bicarbonate 29. Primary respiratory acidosis with metabolic compensation. Correlate with ventilation and work of breathing.
Common mistakes and fast fixes
Using the wrong unit family for PaCO₂. Fix. Convert kilopascal to millimeters of mercury or set the calculator to SI before entry.
Forgetting that a normal pH may hide mixed disorders. Fix. Review PaCO₂ and bicarbonate direction and check expected compensation before you call it normal.
Rounding too early on borderline values. Fix. Enter the digits shown. Compare to the range after the calculator displays the result.
Using an ABG result without clinical context. Fix. Pair the number set with the ventilator settings, oxygen delivery method, and patient state. ABG numbers guide care only when paired with the bedside picture.
Copying a label from a door sticker or old report. Fix. Confirm that the ABG you are reading is current and that the units match your entry fields.
Field notes for busy clinicians
Lead with pH, then name the driver. This keeps the discussion clear and short.
Write one sentence that calls out compensation or a mix when present. This helps handover and plan review.
Check expected compensation when pH and the driver do not line up cleanly. It takes ten seconds and often reveals a second process.
Switch units only when needed. If your team uses millimeters of mercury, stay consistent and convert only the outliers.
Bookmark two things. Calculator page and a brief ABG interpretation reference so the ranges are always one click away.
FAQ
How to calculate ABGs
There is no single calculation, but there is a consistent sequence. Read pH to decide acidemia or alkalemia. Decide the driver by looking at PaCO₂ and bicarbonate. Then check whether the other variable changes in the expected direction. Use a compensation rule such as Winters formula when metabolic acidosis is present.
How to interpret ABGs quickly
Use a five step approach. Identify pH status. Identify the primary disorder by the direction of PaCO₂ or bicarbonate. Check expected compensation. Look for mixed patterns if pH is near normal but the other values are off. Add clinical context before you act.
What are normal ABG values
For adults, pH 7.35 to 7.45, PaCO₂ 35 to 45 millimeters of mercury, and bicarbonate 22 to 26 milliequivalents per liter are typical. Many teaching references use these same bounds. Confirm with your laboratory documentation when needed.
How do I switch between kilopascal and millimeters of mercury
Multiply kilopascal by seven point five zero zero six two to get millimeters of mercury. Multiply millimeters of mercury by zero point one three three three two to get kilopascal. Your ABG calculator can do this internally when you change the unit toggle.
What is Winters formula and when do I need it
In a pure metabolic acidosis, expected PaCO₂ equals one point five times bicarbonate plus eight, with a tolerance of two. If measured PaCO₂ is higher than expected there is a superimposed respiratory acidosis. If lower there is a superimposed respiratory alkalosis. This helps detect mixed disorders.
Does a normal pH mean there is no disorder
No. A normal pH can result from a mixed disorder where one process pushes up and the other pushes down. Review PaCO₂ and bicarbonate and apply a compensation check before you call it normal.
Where can I try an online ABG calculator
Use the live tool here and follow the steps in this guide.
Conclusion and next steps
You can now use an ABG calculator with a clear and safe method. Set the correct unit family. Enter pH, PaCO₂, and bicarbonate carefully. Name the primary disorder. Check expected compensation when appropriate. Write a short interpretation that pairs the numbers with the clinical picture.
Action list for practice.
Pick the correct unit set on the page.
Run two conversions between kilopascal and millimeters of mercury to get fluent.
Analyze two example ABGs and write a one line interpretation for each.
Verify one output against Winters formula to screen for a mixed process.