Estimating the size of an intracerebral hemorrhage fast and reliably matters. An ICH Volume Calculator gives a quick bedside estimate so teams can triage, communicate risk, and track change over time while formal volumetry or advanced tools are not yet available. The most widely used approach is the simple ABC over two method that was validated against planimetry and can be done in under a minute on routine head CT.
ICH Volume Calculator (ABC/2)
Estimate intracerebral hematoma volume from CT. Enter measurements in centimeters (cm) and millimeters (mm). Educational Use
Disclaimer
Instructions: Measure A and B on the slice with the largest hematoma area. Count slices showing hemorrhage using the rule above and multiply by slice thickness to get C (in cm).
Explore more heart calculator:
What an ICH Volume Calculator does
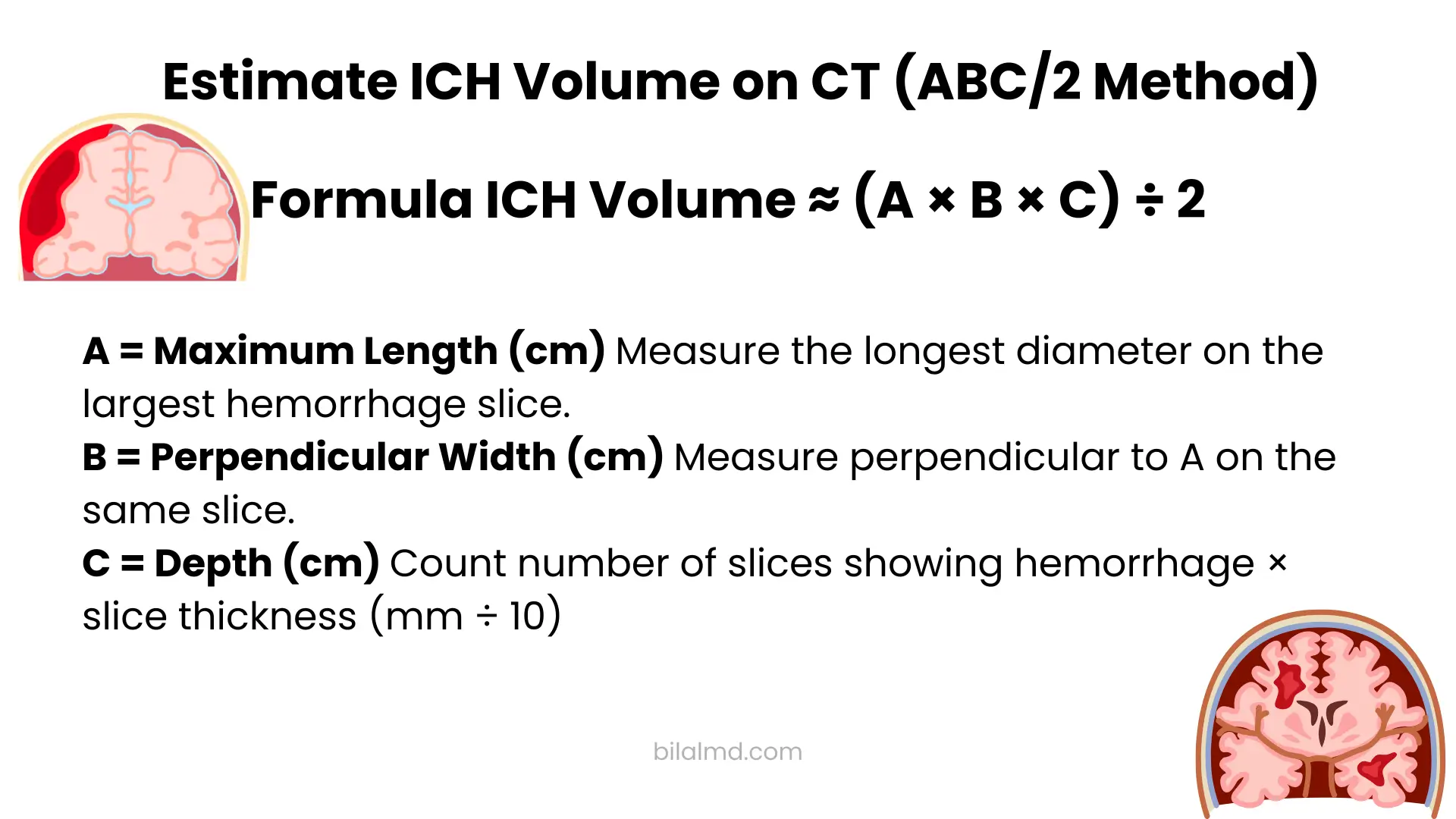
An ICH Volume Calculator converts three CT measurements into a volume in milliliters. The classic rule multiplies the largest diameter of the bleed by the perpendicular diameter on the same axial slice and by the craniocaudal extent, then divides by two. In short, A times B times C divided by two. This bedside rule correlates well with computer assisted volumetry in typical ellipsoid shaped bleeds and remains popular because it is easy to teach and fast to perform.
Why the estimate is useful
Hemorrhage volume is a powerful marker of severity and prognosis. A higher volume is associated with higher mortality, and volume is a component of the widely used ICH Score which helps structure early goals of care conversations and research enrollment. A threshold near thirty milliliters is commonly referenced in risk models from the original work on the score.
How the ich volume calculation works step by step
Step one choose the right slice
Find the axial CT slice with the largest cross sectional area of hemorrhage. Measure A as the largest diameter of the hematoma on that slice. Measure B as the diameter at right angles to A on the same slice. These two numbers are in centimeters.
Step two determine C the craniocaudal extent
Count how many slices show hemorrhage and multiply that count by the slice thickness to get C in centimeters. Many services use a practical half slice rule for partial involvement. A slice with more than seventy five percent involvement counts as one slice, about one quarter to three quarters counts as half a slice, and less than one quarter counts as zero.
Step three calculate the volume
Use the formula A times B times C divided by two. That result in milliliters approximates cubic centimeters. This rule is a simplified version of the ellipsoid volume formula which is pi times A times B times C divided by six when A B and C are full diameters.
A quick example
Suppose A is 5.4 centimeters B is 3.2 centimeters the slice thickness is 5 millimeters and hemorrhage is seen on six slices. C equals 0.5 centimeters times 6 which is 3 centimeters. The ABC over two estimate is 5.4 times 3.2 times 3 divided by two which is about 25.9 milliliters. If you compute the pure ellipsoid reference using pi over six you get a slightly different number which helps explain why real world estimates can be a little above or below perfect planimetry.
When ABC over two is best and when it struggles
The method performs very well for compact bleeds with an ellipsoid look. As the shape becomes irregular or multilobular and as volumes grow larger the rule tends to overestimate compared with planimetry. Several validation studies and reference reviews highlight this pattern and still support the method as a practical first pass.
There has been debate about switching to ABC over three for very irregular shapes. A recent analysis concluded that a global switch is not necessary and that ABC over two remains broadly acceptable even for irregular hematomas, though clinical judgment is required.
Why volume matters in early decisions
Volume feeds into the ICH Score together with factors like location Glasgow Coma Scale intraventricular extension and age. Teams often reference thirty milliliters as a signal for worse prognosis in classic supratentorial bleeds based on the original score work. Volume also helps track change between scans and can inform conversations about transfer level of care and trial eligibility. An ICH Volume Calculator does not replace specialist review but it supports consistent language at the door.
Practical tips to improve accuracy
Measure on the true max area slice
Eyeball the stack and land on the single slice with the largest hematoma area before taking A and B. Small shifts away from the max slice can materially change A times B.
Use the half slice rule consistently
If a slice shows roughly one quarter to three quarters of the area you saw on the reference slice count it as half. This keeps C stable across raters and aligns with widely used calculator instructions.
Check the units
Slice thickness is usually listed in millimeters. Convert to centimeters before multiplying by the slice count. Many mistakes come from mixing units.
Know where the method can mislead
Very lobulated bleeds or those with finger like projections are less ellipsoid so ABC over two can overshoot. Posterior fossa hematomas and bleeds with large intraventricular components can also be tricky. In such situations consider documenting the ABC over two estimate and a qualitative note about shape and consider planimetry or three dimensional software when available.
Use the ellipsoid reference to sanity check
For clean ellipsoid cases the ellipsoid formula pi times A times B times C over six provides a useful cross check. Large gaps between that and ABC over two hint that the bleed geometry may not be a good fit for the shortcut.
Digital tools you can use today
Many teams keep a simple calculator bookmarked on emergency and stroke room workstations. Reputable references outline the same process described here and include reminders about counting partial slices and keeping units straight. These resources are helpful for training and for keeping everyone on one method.
ICH Volume Calculator versus full volumetry
The bedside method exists to get a safe reasonable number quickly. Planimetric and three dimensional software can be more precise, especially for complex shapes, but they take more time and may not be immediately available in acute workflows. Reviews emphasize that ABC over two performs well enough to guide triage and early communication yet caution that it can overestimate larger or irregular bleeds. In short use the shortcut to orient your team then refine with advanced tools when time and resources allow.
Frequently asked questions
How accurate is ABC over two compared with software based volumetry
It correlates strongly with planimetric measurements for small to moderate and fairly compact bleeds and can be completed in well under a minute. The method tends to overestimate volume as the bleed becomes larger or more irregular which is a known tradeoff.
Do I count slices that only show a small sliver of blood
Use the half slice approach that many services teach. Greater than three quarters of the area seen on the max slice counts as one. About one quarter to three quarters counts as half. Less than one quarter counts as zero. This keeps teams consistent and reduces noise between raters.
Should I ever use ABC over three for irregular bleeds
Evidence suggests that a blanket switch to ABC over three is not needed. ABC over two usually remains acceptable even when the shape is irregular. Document the geometry and consider planimetry when the number will drive a high stakes choice.
Does ABC over two include blood in the ventricles
The rule is designed for parenchymal hemorrhage. If there is substantial intraventricular blood note it separately and consider scores that account for intraventricular extension such as the ICH Score.
Can I measure C as a single craniocaudal length instead of counting slices
Yes. Some references accept cranio caudal length in centimeters as C rather than slice count times thickness if that is easier on your viewer. The result should be similar when the bleed is fairly uniform. Consistency within a team matters most.
What volume cutoffs matter clinically
Volume is only one part of prognosis. The ICH Score includes a volume component and many teams pay attention to the thirty milliliter region because higher volumes track with worse outcomes in the original work. Use this in context along with location level of consciousness intraventricular extension and age.
Why does an ellipsoid reference sometimes give a different number
The ABC over two shortcut approximates the ellipsoid formula which is pi times A times B times C divided by six when using full diameters. Differences between the two can flag bleeds that are far from ellipsoid.
Key takeaways
An ICH Volume Calculator gives a fast common language for teams dealing with acute hemorrhage. Measure the largest diameter and its perpendicular on the slice with the most blood. Determine the craniocaudal extent with a consistent approach for partial slices. Multiply A by B by C and divide by two to get a practical number in milliliters. Use that number to orient triage and family communication and to track change, while recognizing that complex or very large bleeds are better served by planimetry or three dimensional tools when possible.