1. Fetal Circulation (before birth)
- Lungs are not working properly before birth.
- The placenta does oxygenation of blood.
- The umbilical cord has:
- 2 arteries
- 1 vein
- The umbilical vein carries approximately 80% oxygenated blood from the placenta to the fetus.
2. Important Shunts (and Adult Remnants)
- Ductus venosus → connects the umbilical vein to the IVC → becomes ligamentum venosum.
- Foramen ovale → shunts blood RA → LA → becomes fossa ovalis.
- Ductus arteriosus → connects pulmonary artery to aorta → becomes ligamentum arteriosum.
congenital heart diseases
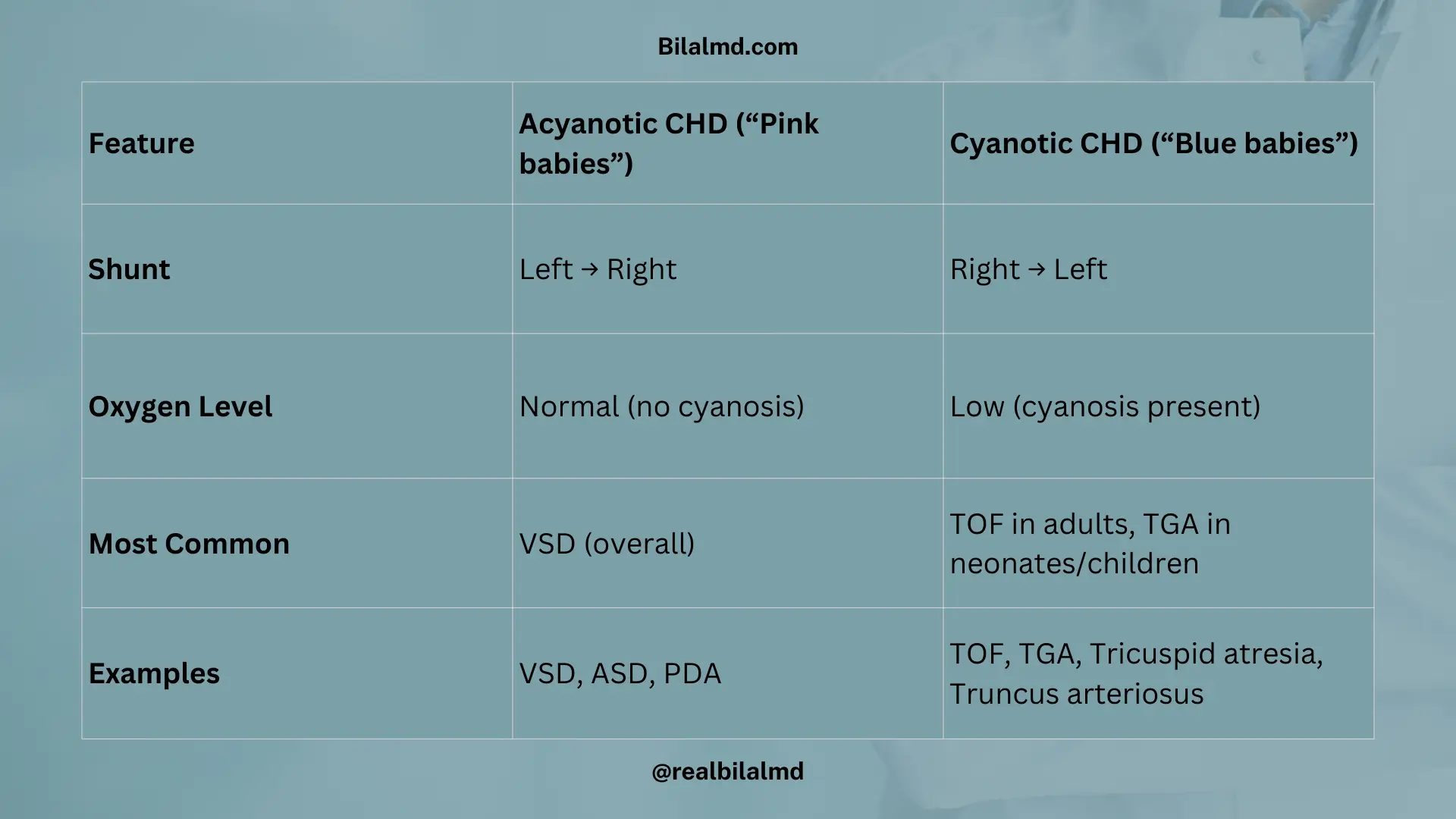
| Feature | Acyanotic CHD (“Pink babies”) | Cyanotic CHD (“Blue babies”) |
|---|---|---|
| Shunt | Left → Right | Right → Left |
| Oxygen level | Normal (no cyanosis) | Low (cyanosis present) |
| Most common | VSD (overall most common CHD) | TOF in adults, TGA in children |
| Examples | VSD, ASD, PDA | TOF, TGA, Tricuspid atresia, Truncus arteriosus |
1. Acyanotic Heart Diseases (L → R Shunt, “Pink Babies”)
General Features
- Blood flow: Left → Right shunt → mixing of oxygenated with deoxygenated blood.
- Symptoms: May appear late.
- Complication: Backward reversal of shunt → Eisenmenger syndrome (cyanosis develops).
1. Patent Ductus Arteriosus (PDA)
Causes:
- Maternal rubella infection
- Maternal ↑ prostaglandins
Auscultation: Machine-like murmur
Pulse: Wide pulse pressure
Management:
- Indomethacin → closes duct
- Prostaglandins (PGE1) → keep it open
- If not closed by 8 months → surgery
Special note: PDA must not be closed in TOF and TGA (cyanotic CHD).
2. Atrial Septal Defect (ASD)
- Shunt: Left → Right
- Auscultation: Wide, fixed splitting of S2
3. Ventricular Septal Defect (VSD)
- Shunt: Left → Right
- CXR: Cardiomegaly, delayed closure of the pulmonary valve
- Complications: Pulmonary arterial hypertension (PAH)
- Association: Down syndrome
- Investigation of choice: Echocardiography
- Types:
- Restrictive VSD → often closes spontaneously
- Non-restrictive VSD → symptoms: fatigue, poor growth, failure to thrive, malaise
- Auscultation: Harsh holosystolic murmur
- Treatment: Surgical closure
2. Cyanotic Heart Disease
Tetralogy of Fallot (TOF)
Mnemonic – PROV
- P → Pulmonary stenosis / Pulmonary hypertension
- R → Right ventricular hypertrophy (RVH)
- O → Overriding of the aorta
- V → Ventricular septal defect (VSD)
The most common cyanotic CHD in children
Clinical features
- Usually presents at 8–14 years
- Dyspnea
- Bluish discoloration (cyanosis)
- Squatting → increases systemic vascular resistance → improves oxygenation
Investigations
- X-ray: Boot-shaped heart
- ECG: RVH + Cardiomegaly
Treatment
Definitive: Surgical repair
Here are other materials for NLE NRE step 1
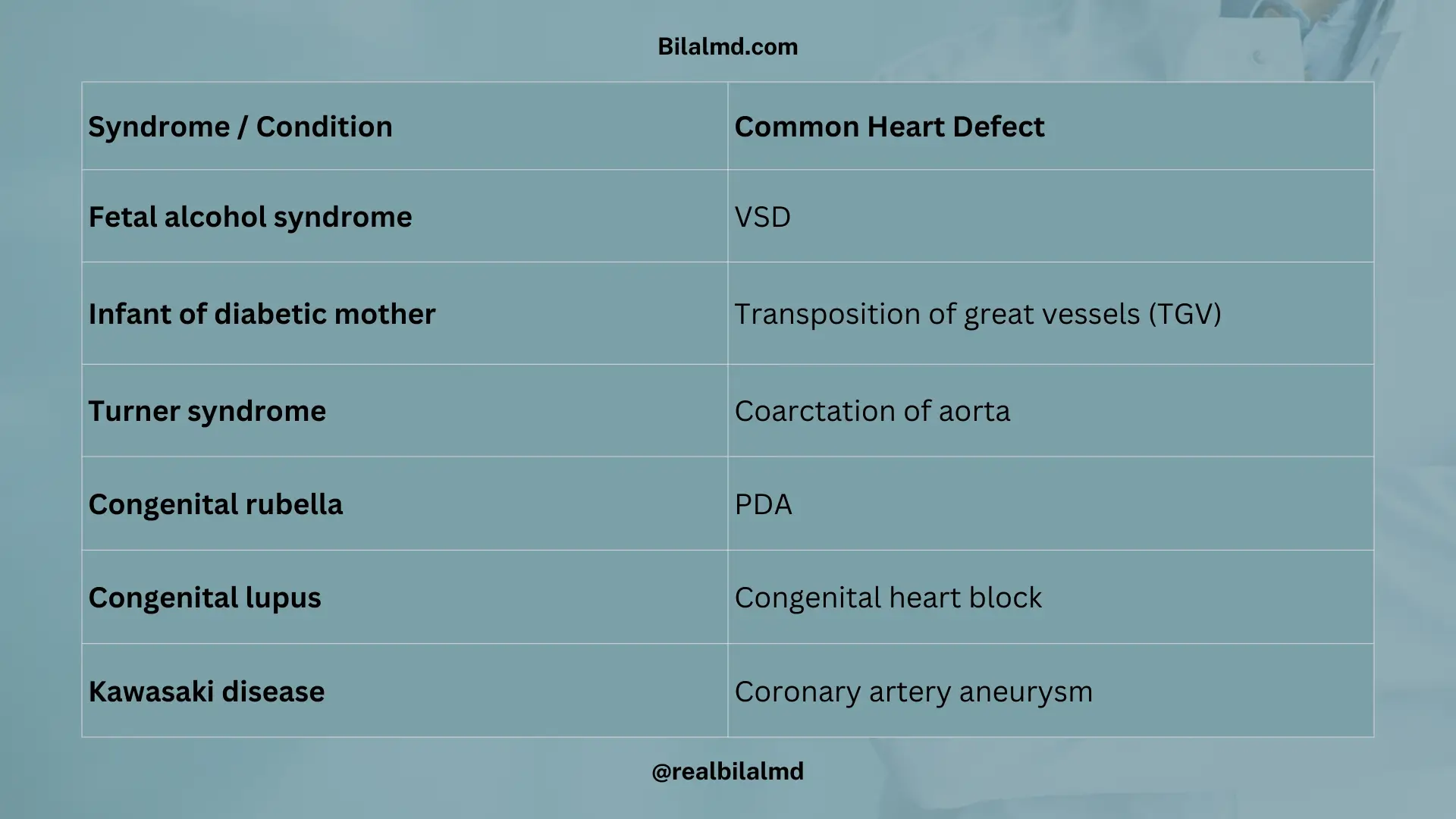
1. CHD Associations with Conditions
- Fetal alcohol syndrome → VSD
- Infant of a diabetic mother → Transposition of great vessels (TGV)
- Turner syndrome → Coarctation of the aorta
- Congenital rubella → PDA
- Congenital lupus → Congenital heart block
- Kawasaki disease → Coronary artery aneurysm
2. Classic X-ray Appearances
- TOF → Boot-shaped heart
- TGV → Egg-on-a-string (Egg shell)
3. Congenital Heart Diseases – Murmurs & Sounds
| Condition | Characteristic Murmur / Sound |
|---|---|
| VSD | Harsh holosystolic murmur |
| ASD | Wide, fixed splitting of S2 |
| PDA | Continuous “machine-like” murmur |
3. Coarctation of Aorta
Narrowing of the aorta → ↑ blood flow in upper extremities & ↓ flow in lower extremities
Types
| Feature | Pre-ductal Coarctation | Post-ductal Coarctation |
|---|---|---|
| Site of narrowing | Distal to the ductus arteriosus | Hypertension in the upper limbs, radio-femoral delay |
| Age group | Infants / < 5 years | Children & adolescents > 5 years |
| Severity | Severe → early presentation | Less severe → later presentation |
| Association | Turner syndrome | Bicuspid aortic valve |
| Clinical course | Early cyanosis, heart failure, poor growth | Hypertension in the upper limbs, radio-femoral delay |
| Prognosis | Needs urgent intervention | May present later, diagnosed on routine BP check |
Clinical Features
- Upper extremities: Hypertension, redness
- Lower extremities: Hypotension, cyanosis, poor growth, failure to thrive
Blood Pressure:
- ↑ SBP in arms
- ↓ SBP in legs
Pulse: Radio-femoral (radio-temporal) delay
Investigations
- CXR
- Echo with color Doppler (diagnosis of choice)
Management
- PGE1 infusion → keep ductus arteriosus open (in infants)
- Balloon angioplasty → definitive treatment
4. Chromosomal disorder
| Syndrome | Chromosome / Karyotype | Causes | Clinical Features | Associations | Prognosis / Treatment |
|---|---|---|---|---|---|
| Down Syndrome (Trisomy 21) | 47, +21 | – Meiotic nondisjunction (↑ risk with maternal age) – Robertsonian translocation – Mosaicism | – Intellectual disability – Flat nasal bridge – Hypotonia (floppy baby) – Single palmar crease – Sandal gap deformity – Poor growth, short stature | – Duodenal atresia (“double bubble sign”) – Hirschsprung disease – CHD (VSD > ASD) – Early Alzheimer’s – ↑ Risk of ALL & AML | Supportive therapy; multidisciplinary care |
| Edward Syndrome (Trisomy 18) | 47, +18 | Meiotic nondisjunction | – Low-set ears – Rocker-bottom feet – Clenched fists (overlapping fingers) – Micrognathia – Prominent occiput | Horseshoe kidney | 45, X0 |
| Patau Syndrome (Trisomy 13) | 47, +13 | Meiotic nondisjunction | – Polydactyly – Microphthalmia – Microcephaly – Holoprosencephaly – Cleft lip/palate – Cutis aplasia | CHD, CNS malformations | Die within 1 year |
| Turner Syndrome | Coarctation of the aorta Horseshoe kidney | Monosomy X (sex chromosome loss) | – Short stature – Webbed neck – Wide-spaced nipples – Primary amenorrhea – Streak ovaries – Lymphedema of hands/feet | 47, XXY | Estrogen therapy (induces puberty, protects bone health) |
| Klinefelter Syndrome | ↑ Risk of breast cancer & autoimmune diseases | Extra X in males (↑ maternal age risk) | – Tall male – Hypogonadism – Oligospermia/infertility – Testicular atrophy – Gynecomastia – Female-type hair distribution | ↑ Risk breast cancer & autoimmune diseases | Testosterone replacement therapy |
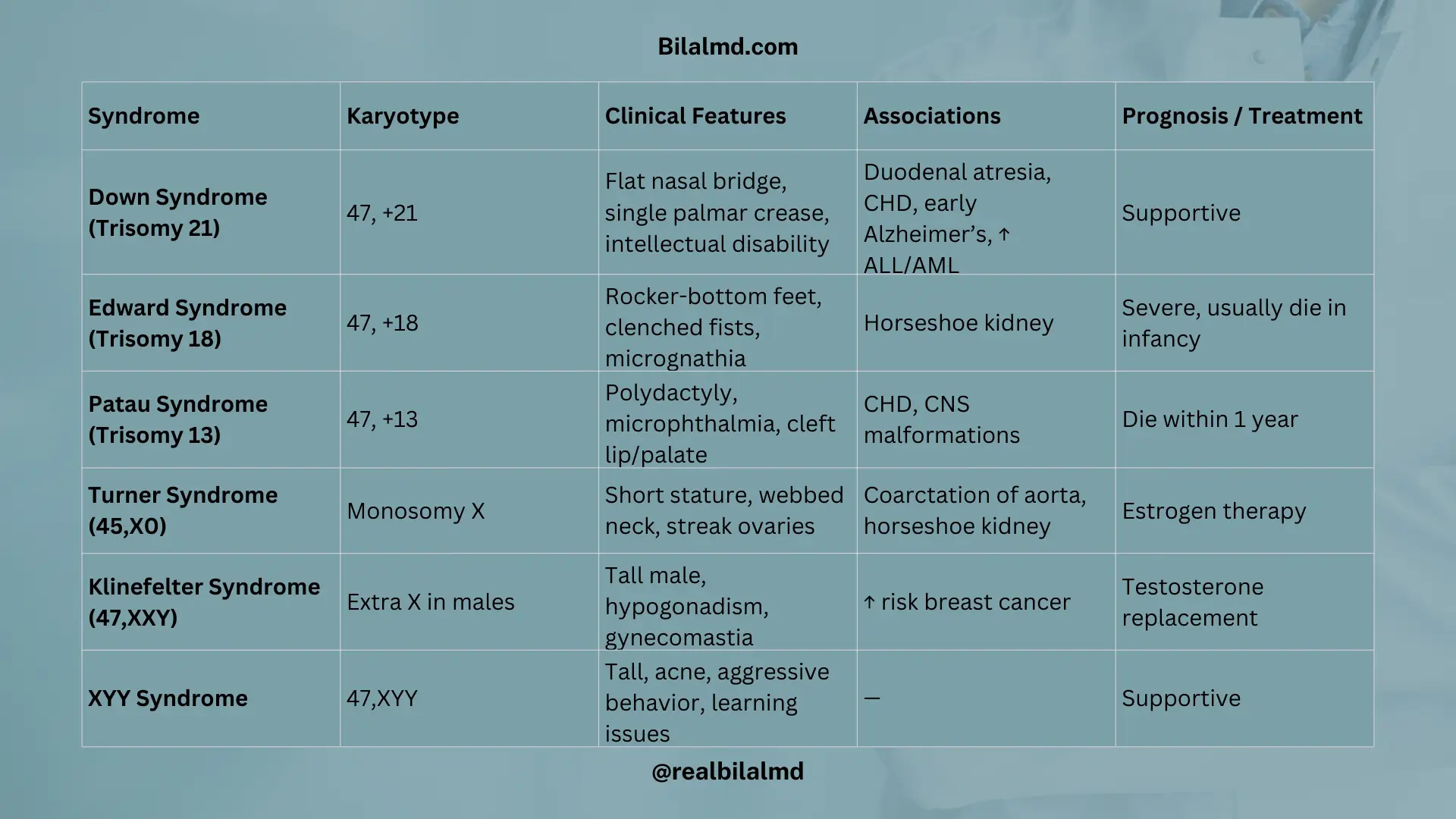
5. Double Y Chromosome (47, XYY)
Karyotype: 47, XYY
Cause: Meiotic nondisjunction (usually paternal)
Clinical Features:
- Normal height and physical development
- Frequent anger / aggressive behavior
- Severe acne
- May have mild learning difficulties
Management: Supportive care, behavioral counseling if needed
6. Hypertrophic Pyloric Stenosis
- Definition: Hypertrophy and narrowing of the pyloric sphincter → delayed gastric emptying
- Risk Factors:
- Exact cause unknown
- Maternal erythromycin exposure
- Clinical Features:
- Non-bilious projectile vomiting (classic)
- Infant remains hungry after vomiting (“hungry vomiter”)
- Signs of dehydration
- Examination:
- Abdominal distension
- Olive-shaped, mobile, non-tender mass in the epigastrium
- Investigations:
- Metabolic alkalosis (hypochloremic, hypokalemic)
- Barium swallow → “string sign”
- Treatment:
- Initial: NPO (nil per os), IV fluids, correct electrolytes
- Definitive: Surgical pylorotomy
7. Intussusception
- Proximal intestine telescopes into the distal part → bowel obstruction
- Age group: 6 months – 3 years
- Epidemiology: More common in boys
- Clinical Triad:
- Intermittent abdominal pain
- Bloody diarrhea (“red currant jelly stools”)
- Vomiting
- Investigations:
- USG abdomen: “Target sign / Doughnut sign” at the site of pain
- ABG: Metabolic alkalosis (due to vomiting)
- Treatment:
- Initial: Air or barium enema (diagnostic + therapeutic)
- Surgery if enema fails or perforation is suspected
8. Meckel’s Diverticulum
- Failure of the omphalomesenteric (vitelline) duct to obliterate → true diverticulum
- Epidemiology: More common in males
- Rule of 2’s:
- 2% of the population
- 2 times more common in boys
- 2 inches in length
- 2 feet from the ileocecal valve
- 2 types of ectopic mucosa (gastric & pancreatic)
- Symptoms before 2 years of age
- Clinical Features:
- Often asymptomatic
- Painless hematochezia (classic)
- Pallor, shortness of breath due to anemia
- Investigations:
- Technetium-99m pertechnetate scan → detects ectopic gastric mucosa
- Treatment: Surgical resection
9. Hirschsprung Disease
- Absence of ganglion cells in the intestinal wall (neural crest cell migration defect) → no peristalsis in the affected segment.
- Epidemiology / Risk Factors:
- Male > Female
- Premature infants
- Associated with Down syndrome
Clinical Features
- Delayed passage of meconium (>48 hours after birth)
- Bilious vomiting
- Abdominal distention
- Failure to thrive
Examination
- DRE: Explosive discharge of stool & gas → squirt sign
Diagnosis
- Gold standard: Rectal biopsy → absence of ganglion cells
- Supportive: Contrast enema showing transition zone
Treatment
- Surgical resection of the aganglionic segment (pull-through procedure)
Key Differentiation in Delayed Meconium
- If respiratory symptoms present → think Cystic Fibrosis
- If no respiratory symptoms:
- DRE → gush of stool → Hirschsprung disease
- DRE → no stool → Other intestinal obstruction (e.g., ileal atresia, meconium ileus in CF)
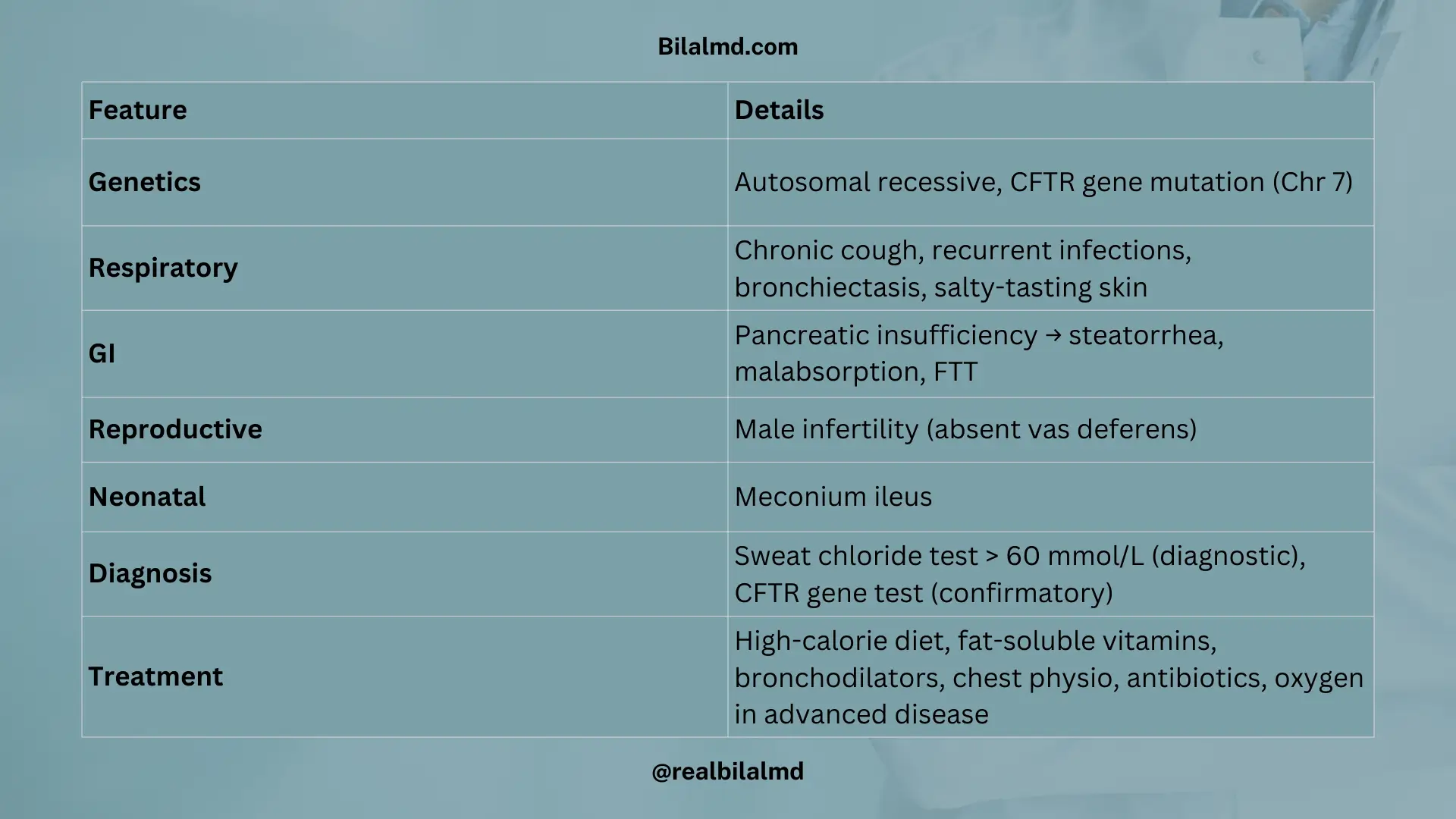
10. Cystic Fibrosis (CF)
- Genetics:
- Autosomal recessive
- Mutation in the CFTR gene (Chromosome 7)
Clinical Features
- Respiratory:
- Chronic cough, recurrent lung infections
- Wheeze, bronchiectasis
- Salty-tasting skin (due to high NaCl in sweat)
- Gastrointestinal:
- Pancreatic insufficiency → malabsorption, steatorrhea, FTT (failure to thrive)
- Delayed passage of meconium (meconium ileus) in neonates
- Other:
- Male infertility (absence of vas deferens)
Diagnosis
- Sweat chloride test: > 60 mmol/L = diagnostic
- Genetic testing for CFTR mutation (confirmatory)
Treatment
- Nutritional:
- High-calorie, high-protein diet
- Supplement fat-soluble vitamins (A, D, E, K)
- Pulmonary:
- Bronchodilators
- Anti-inflammatory drugs
- Antibiotics (for recurrent infections)
- Chest physiotherapy
- Oxygen supplementation in advanced disease
11. Kawasaki Disease
A multi-segment, medium-vessel vasculitis, primarily affecting children < 5 years. Considered an autoimmune phenomenon.
Phases
- Acute phase (1–2 weeks):
- High fever > 5 days
- Rash, conjunctivitis, strawberry tongue, lymphadenopathy, extremity changes
- ↑ Risk of myocarditis
- Subacute phase (2–8 weeks):
- Desquamation (peeling of skin on fingers/toes)
- ↑ Risk of coronary artery aneurysm
- Chronic phase:
- Gradual resolution of symptoms
- ESR and CRP return to normal
Clinical Features (Mnemonic: CRASH & Burn)
- Conjunctivitis (bilateral, non-purulent)
- Rash (polymorphous)
- Adenopathy (cervical, usually unilateral)
- Strawberry tongue + mucosal changes (red, cracked lips)
- Hand and foot changes (edema, erythema, peeling)
- Burn: Fever > 5 days
Treatment
- High-dose Aspirin (anti-inflammatory, antipyretic, antiplatelet)
- IVIG (prevents coronary aneurysm if given early)
- Low-dose Aspirin (continued up to 6 weeks or longer if coronary involvement persists)
- Corticosteroids (for refractory disease)
12. Juvenile Idiopathic Arthritis (JIA)
- Autoimmune disease → joint inflammation
- Morning stiffness + gradual loss of movement
- Symptoms last ≥ 6 weeks
- Age: < 16 years
Types
| Type | Key Features |
|---|---|
| Pauciarticular JIA | Few joints (≤ 4) No systemic symptoms Uveitis (slit lamp exam) ANA (+), RF (–) |
| Polyarthritis JIA | ≥ 5 joints involved Systemic symptoms present |
| Systemic JIA | Triad → Salmon pink rash, Hepatosplenomegaly, High grade fever ANA (–), RF (–) |
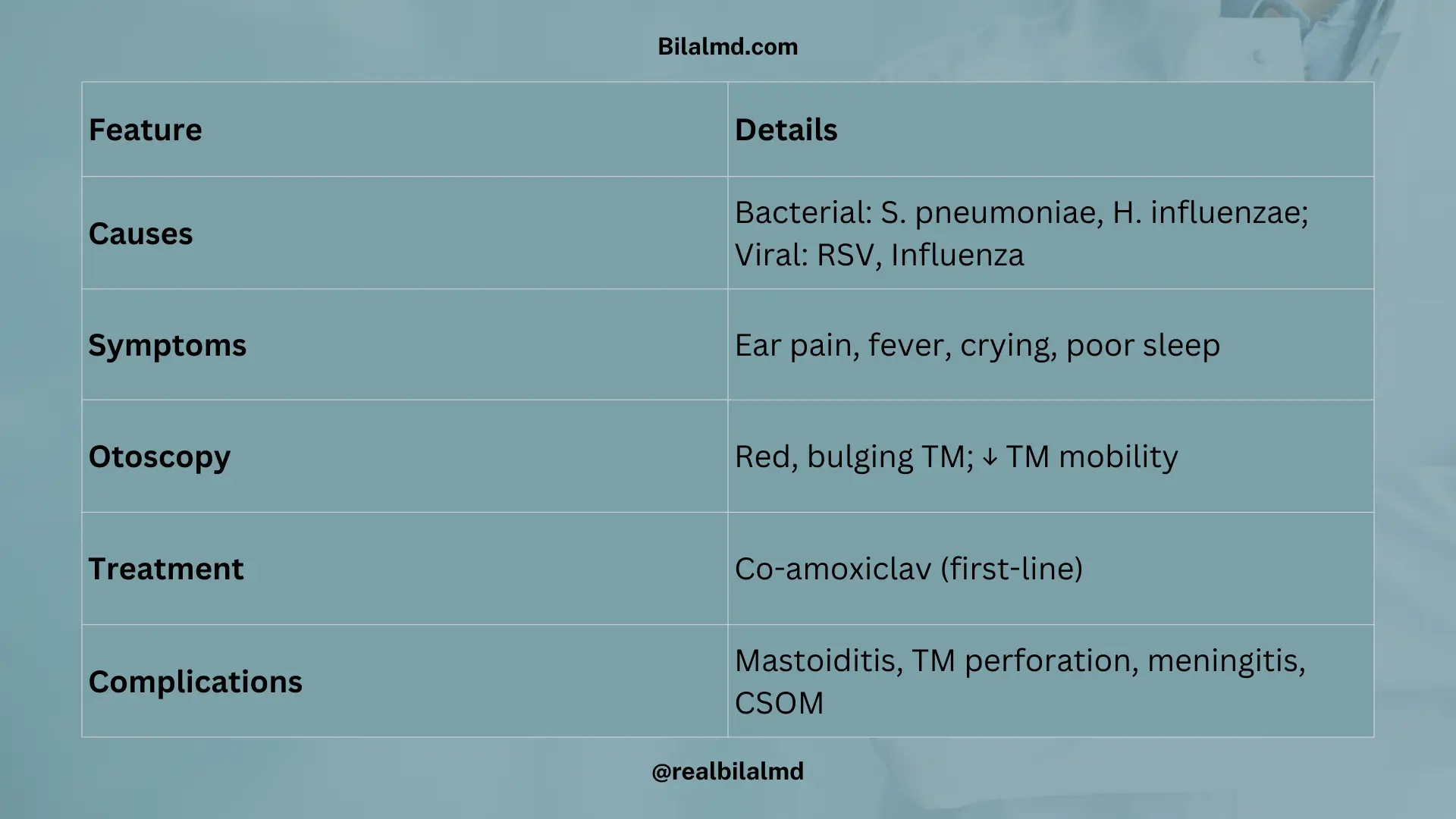
13. Acute Otitis Media (AOM)
Inflammation of the middle ear cavity.
Causes:
- Bacterial: Streptococcus pneumoniae, Haemophilus influenzae
- Viral: Measles, Influenza, RSV
- Non-infectious: Allergy
Clinical Features:
- Otalgia (ear pain)
- Fever
- Excessive crying
- Difficulty sleeping
Otoscopic Findings:
- Erythematous tympanic membrane (TM)
- Bulging or retraction of TM
- Decreased TM mobility
Treatment:
- First line: Co-amoxiclav
Complications (if untreated):
- Mastoiditis
- TM perforation → conductive hearing loss
- Meningitis
- Chronic suppurative otitis media (CSOM)
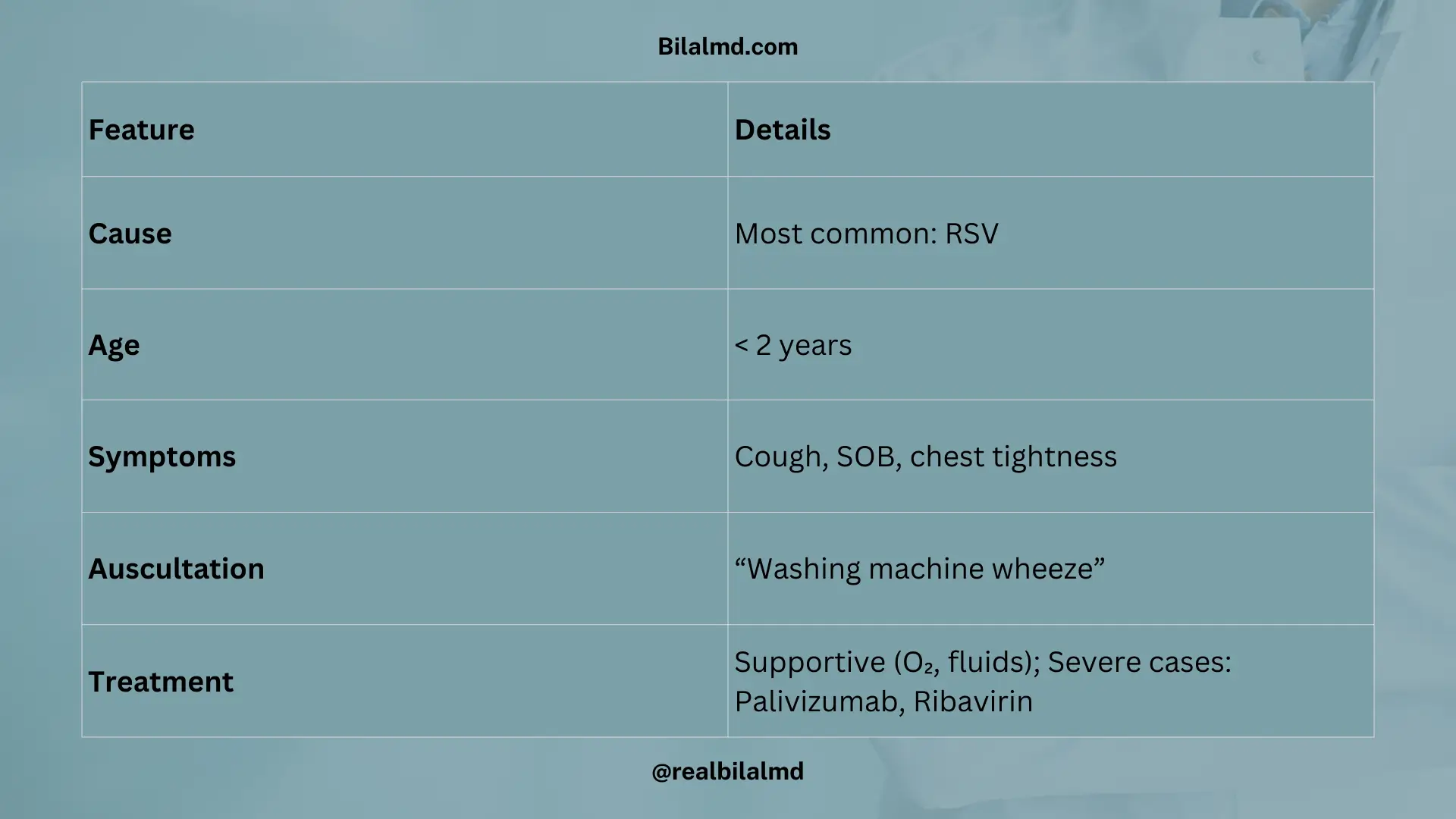
14. Bronchiolitis
Inflammation of small airways, usually in children < 2 years.
Cause:
- Most common: Respiratory Syncytial Virus (RSV)
Clinical Features:
- Cough
- Dyspnea, shortness of breath
- Chest tightness
- Auscultation: “Washing machine wheeze”
Treatment:
- Primarily supportive care
- Resistant/severe cases: Palivizumab, Ribavirin
15. Meningitis
Causes (Age-wise):
- Neonates: Group B Streptococcus (Streptococcus agalactiae)
- Infants: Streptococcus pneumoniae
- Adolescents (14–18 yrs): Neisseria meningitidis
- Middle-aged adults: Streptococcus pneumoniae
- Viral: HSV (Herpes Simplex Virus)
- Fungal: Cryptococcus neoformans
Clinical Signs:
- Kernig’s sign (+)
- Brudzinski’s sign (+)
Treatment:
- Ampicillin + Cefotaxime