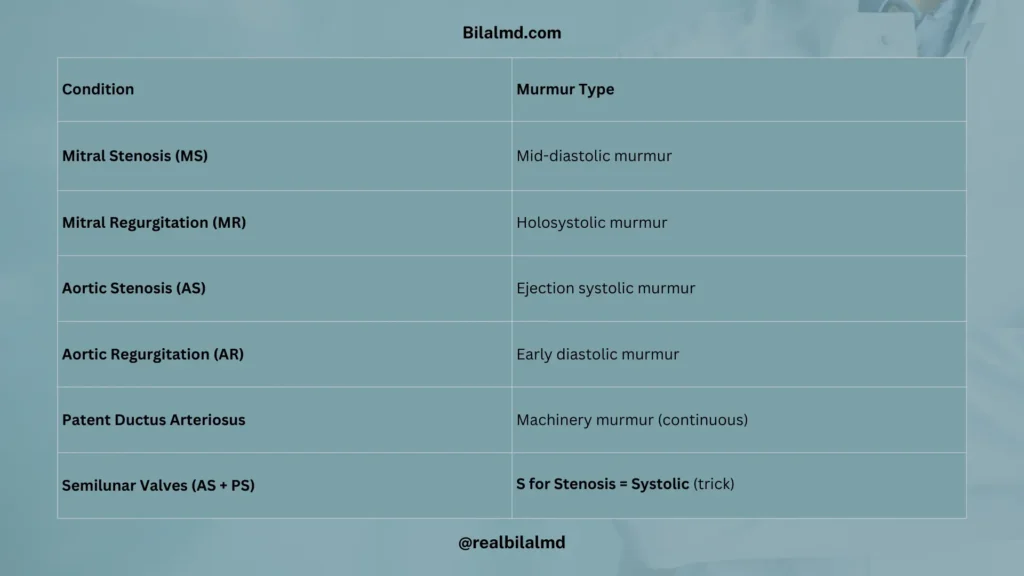
1. Cardiac Murmur
| Condition | Murmur Type |
|---|---|
| Mitral Stenosis (MS) | Mid-diastolic murmur |
| Mitral Regurgitation (MR) | Holosystolic murmur |
| Aortic Stenosis (AS) | Ejection systolic murmur |
| Aortic Regurgitation (AR) | Early diastolic murmur |
| Patent Ductus Arteriosus (PDA) | Machinery murmur (continuous) |
| Semilunar Valves (Aortic + Pulmonic) | S for Stenosis = Systolic |
2. Rheumatic Fever
Typical Case: Young female, h/o sore throat (1 week ago) → joint pain, chest pain, subcutaneous nodules.
Diagnosis: Jones Criteria (major + minor).
3. Infective Endocarditis
Typical Case: High-grade fever + new-onset murmur.
| Situation | Common Cause |
|---|---|
| After Dental procedure | Strep viridans |
| Damaged valve | Strep viridans |
| Native valve (healthy) | Staph aureus |
| Skin infection source | Staph aureus |
| Prosthetic valve | Staph epidermidis |
| Colon cancer association | Strep bovis (S. gallolyticus) |
Diagnosis
Echocardiography (vegetations, valve damage).
4. Coronary Artery Disease (CAD)
Myocardial Ischemia
- Without necrosis → Angina
- With necrosis → Myocardial Infarction (MI)
- ↑ Cardiac markers
- Coagulation necrosis on pathology
| Marker | Key Point |
|---|---|
| Troponin I | Most specific for MI |
| Troponin T | Most sensitive for MI |
| CK-MB | Used to detect reinfarction (because it rises & falls quickly) |
1. ECG Elevation & MI Localization
| ECG Leads | MI Location | Artery Involved |
|---|---|---|
| V1 – V4 | Anteroseptal wall MI | LAD (branch of LCA) |
| II, III, aVF | Inferior wall MI | RCA (marginal artery) |
| V5, V6, aVL | Lateral wall MI | LCX (branch of LCA) |
Complication
- Post-MI autoimmune pericarditis
- Occurs ~2 weeks after MI
- Known as Dressler Syndrome

2. Heart Block (AV Block)
| Type | ECG Finding | Key Point |
|---|---|---|
| 1st Degree | Constant prolonged PR interval, no missed beats | Benign |
| 2nd Degree – Mobitz I (Wenckebach) | Progressive ↑ PR → then 1 dropped QRS | Usually benign |
| 2nd Degree – Mobitz II | Constant PR, sudden dropped QRS | Risk of progression → Pacemaker needed |
| 3rd Degree (Complete Block) | Atria & ventricles beat independently (P waves unrelated to QRS) | Pacemaker required |
Association
Lyme disease → Can cause Complete Heart Block
3. Cardiomyopathy
1. Dilated Cardiomyopathy (90%)
- Causes: Beriberi, Doxorubicin, Trastuzumab
- Pathology: Systolic failure
- Heart sound: S3
2. Hypertrophic (HOCM, 5–7%)
- Inheritance: Autosomal dominant
- Mutation: β-myosin heavy chain
- Presentation: Young athlete, sudden death
- Pathology: Diastolic failure
- Heart sound: S4
3. Restrictive (2–3%)
- Causes: Hemochromatosis, Amyloidosis
4. Hypertension
- Definition: SBP > 140 mmHg or DBP > 90 mmHg
- Primary (Essential) HTN = Idiopathic, 95%
- Secondary HTN = Identifiable cause, 5%
1. Hypertensive Crisis
- Urgency → No end-organ damage
- Emergency → End-organ damage present
2. Renin-Angiotensin
- Angiotensin I → Angiotensin II by ACE
- ACE inhibitors (-pril)
- Side effects: Cough, Angioedema
| Drug | Key Point |
|---|---|
| Esmolol | Short-acting, used in OT |
| Metoprolol | May cause dyslipidemia |
| Propranolol | Contraindicated in asthma |
| Labetalol, Carvedilol | Block α + β |
5. Anti-arrhythmic Drugs
1. Class I – Na⁺ Channel Blockers
| Subclass | Drugs | Key Points / Side Effects |
|---|---|---|
| 1A | Procainamide, Quinidine, Disopyramide | – SLE-like symptoms (Procainamide) – Cinchonism (Quinidine: tinnitus, dizziness) – Can worsen HF |
| 1B | Phenytoin, Lidocaine | – Best in MI (post-arrhythmia) – Contraindicated in other settings |
| 1C | Propafenone, Flecainide | – Potent, ↑ pro-arrhythmic risk |
2. Class II – β Blockers
- Reduce sympathetic activity
- Examples: Metoprolol, Propranolol, Esmolol
3. Class III – K⁺ Channel Blockers
Mnemonic: AIDS
- Amiodarone
- Ibutilide
- Dofetilide
- Sotalol
4. Class IV – Ca²⁺ Channel Blockers
Verapamil
5. Other Drugs / Notes
- Diphenhydramine → Can cause Angioedema
- Statins
- Inhibit HMG-CoA reductase → ↓ Mevalonate → ↓ Cholesterol
- Side effect: Hepatotoxicity
- HMG-CoA synthase → Produces Ketone bodies
6. Congestive Heart Failure (CHF)
- Normal cardiac output: ~5 L/min
Right-Sided HF
- Raised JVP
- Hepatosplenomegaly
- Ascites
Left-Sided HF
- SOB, Dyspnea, Cough
- On auscultation: Crackles / Rales
- Treatment: Diuretics (Lasix = Furosemide)
7. Cardiac Tamponade
- Definition: Impaired diastolic filling of the heart due to pericardial fluid compression
- Cause: Can occur as a complication of MI
Clinical Features (Beck’s Triad)
- Hypotension
- Muffled heart sounds
- Raised JVP
Treatment
- Pericardiocentesis
8. Heart Sounds
S1 → Closure of AV valves (Mitral + Tricuspid)
S2 → Closure of Semilunar valves (Aortic + Pulmonic)
S3 (Ventricular Gallop)
- Normal: Children, Athletes, Pregnancy
- Abnormal: Dilated cardiomyopathy (↑ LV filling pressure)
- Represents: Rapid filling phase (LV ← LA) → ventricular vibration (“atrial kick”)
Here are other materials for NLE NRE step 1
Check your NRE Step 1 result after completing the exam.