Digestive System (GIT) – Medicine
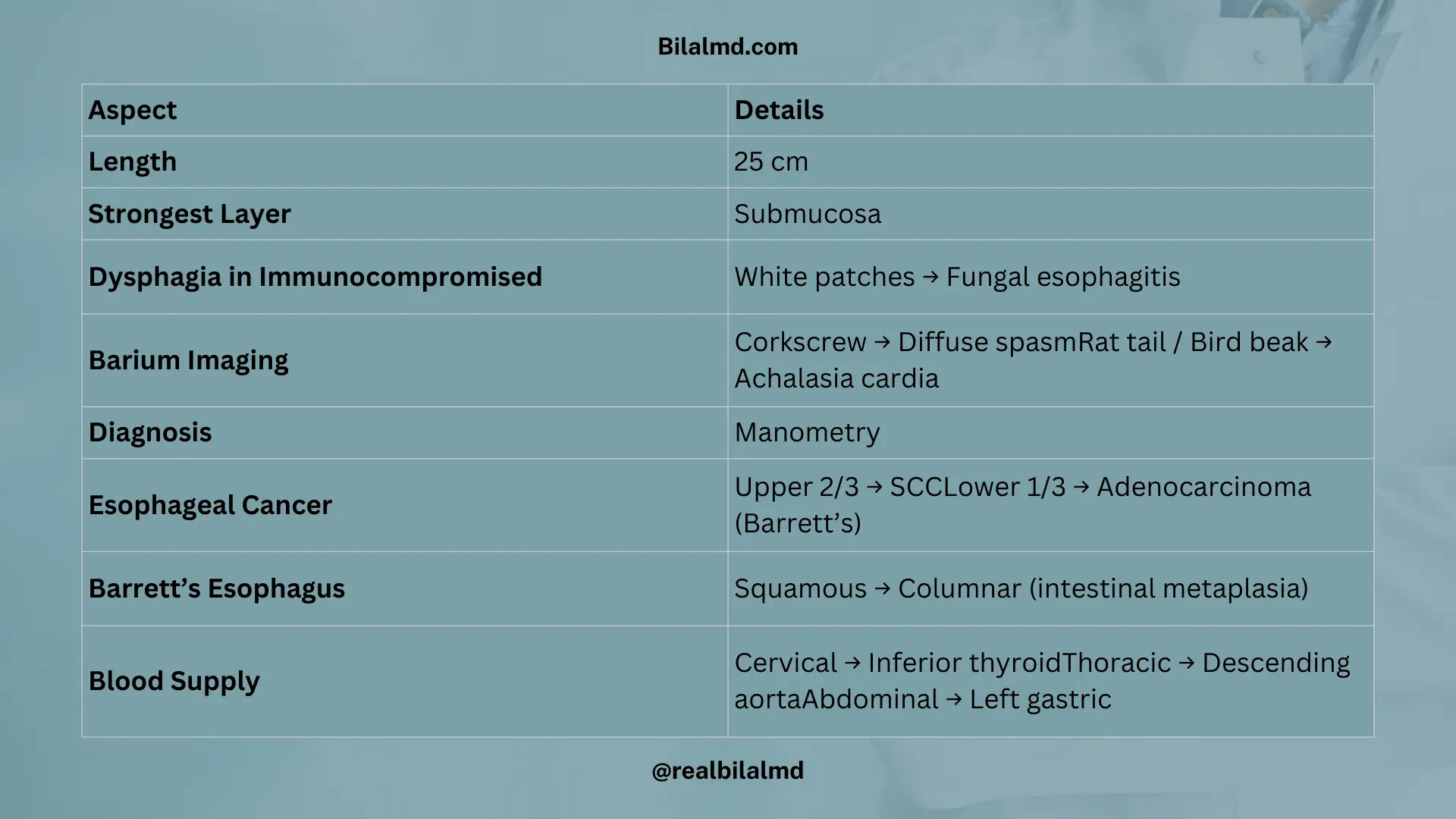
Esophagus: Length: 25 cm long.
Strongest Layer: Submucosa.
Immunocompromised + Dysphagia + Endoscopy: White patches on endoscopy indicate fungal infection, likely fungal esophagitis.
Symptoms:
- Dysphagia (difficulty swallowing) and early sensation of fullness.
Barium Imaging:
- Corkscrew esophagus: Associated with diffuse spasm.
- Rat tail / Bird beak: Indicates achalasia cardia.
Diagnosis:
- Manometry (measures pressure in the esophagus) is used for diagnosis.
Esophageal Cancer:
- 2/3 of esophagus: Squamous cell carcinoma (SCC).
- 1/3 of esophagus: Adenocarcinoma, typically in Barrett’s esophagus.
Barrett’s Esophagus:
- Squamous epithelium to columnar epithelium transformation is intestinal metaplasia. This condition is a precursor to adenocarcinoma.
| Region | Arteries |
|---|---|
| Cervical | Inferior thyroid artery, subclavian artery |
| Thoracic | Descending aorta |
| Abdominal | Left gastric artery |
2. Stomach
Shape: J-shaped organ.
Cells in the Stomach:
- Chief Cells:
- Secrete pepsinogen, which is converted to pepsin to aid in protein digestion.
- Parietal Cells:
- Secrete HCl (Hydrochloric acid), which activates pepsinogen into pepsin and helps with digestion.
- Also release the intrinsic factor, which is crucial for the absorption of Vitamin B12 in the small intestine.
Effect of HCl and Mucosa on Ulcers:
- Increased HCl:
- Can lead to duodenal ulcers, with epigastric pain decreasing after eating.
- Decreased Mucosa:
- Leads to gastric ulcers, causing epigastric pain that increases after eating.
3. H. pylori Testing
- Serum: Detects antibodies.
- Stool Antigen: Detects antigens in stool.
- Urea Breath Test: Measures carbon dioxide after ingesting urea.
Treatment (Tx):
PPI + Antibiotics + Clarithromycin.
4. Epigastric pain
| Condition | Symptom | Outcome |
|---|---|---|
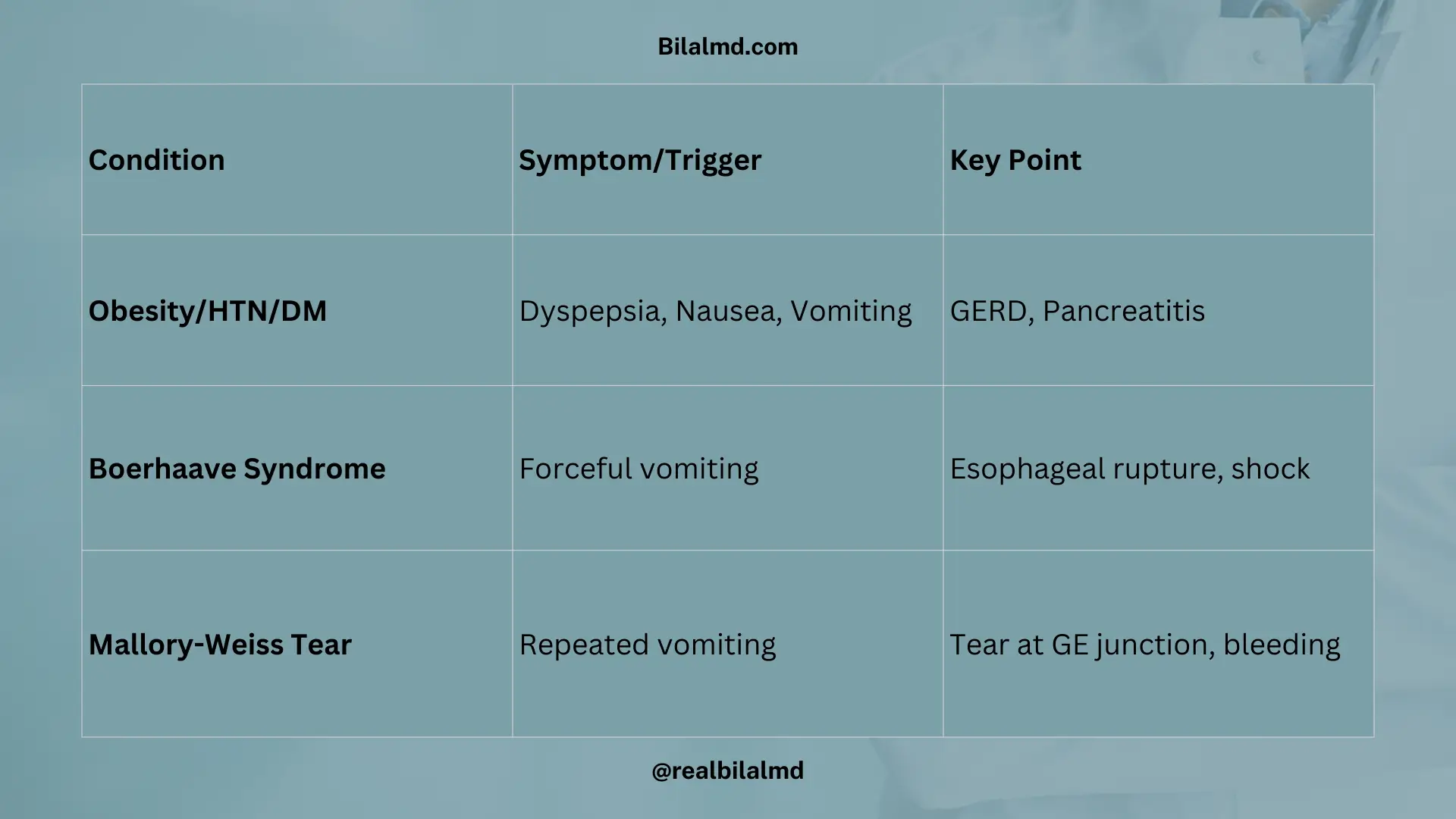
| Obese | Heart burn | Pain radiates to back side |
| HTN | Dyspepsia | Nausea + Vomit |
| DM | Dyspepsia | Nausea + Vomit |
| Chest heaviness in MI | GERD | Acute pancreatitis |
| Condition | Cause/Trigger | Description |
|---|---|---|
| Boerhaave Syndrome | Older age + Shock | Spontaneous esophageal rupture, often following forceful vomiting. |
| Mallory-Weiss Tear | Forceful vomiting | Tear at the esophagus-stomach junction causing bleeding. |
5. Gastric adeno carcinoma
Risk Factors:
- Spicy diet
- Alcohol consumption
- Smoking
- H. pylori infection
- Chronic gastritis
Symptoms:
- Often asymptomatic initially
- Dyspepsia (indigestion)
- Weight loss
Metastasis/Signs
| Syndrome | Affected Node |
|---|---|
| Virchow’s node | Left supraclavicular node |
| Sister Mary Joseph nodule | Around umbilicus |
| Krukenberg tumor | Ovaries |
Patient with Right Lower Abdominal Pain:
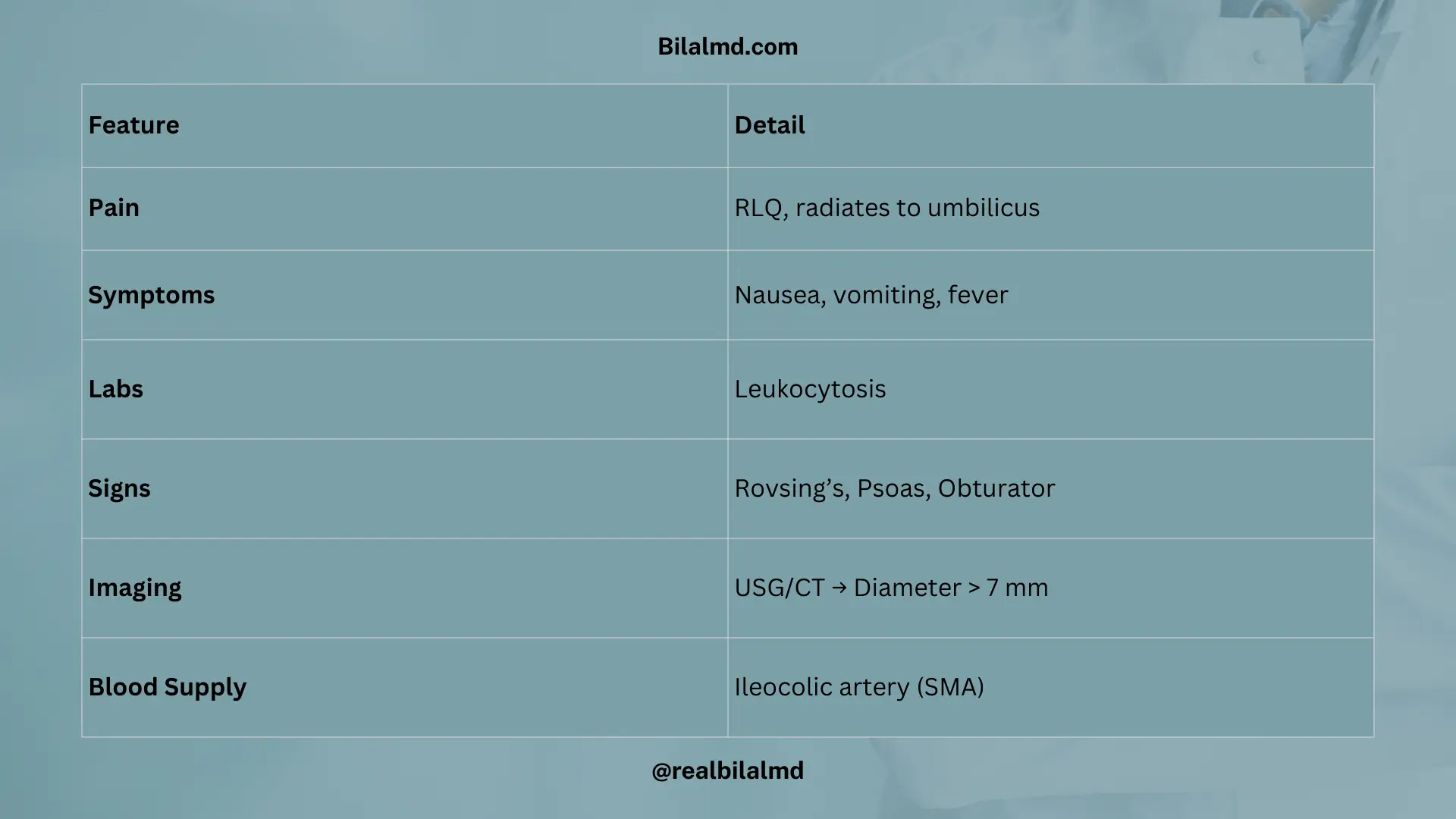
- Diagnosis: Acute Appendicitis.
- Pain Radiation: Radiates to the umbilicus.
- Symptoms: Nausea, vomiting, fever.
- Lab Findings: Leukocytosis (elevated white blood cell count).
| Condition/Sign | Details |
|---|---|
| Appendix Position | Retrocecal (behind the cecum) |
| Appendicular Blood Supply | Ileocolic artery from the Superior Mesenteric Artery (SMA) |
| Rovsing’s Sign | Pain in the right lower quadrant when pressure is applied to the left |
| Psoas Sign | Pain with hip extension; if less than 4, considered normal |
| Obturator Sign | Pain when the hip is flexed and rotated; if 4-7, further observation needed |
| Imaging (USG/IOC) | Appendix diameter > 7 mm is more likely to indicate acute appendicitis |
| Metastasis in Appendiceal Cancer | Spread to supramesenteric lymph nodes |
6. Acute Mesenteric Ischemia
| Condition | Details |
|---|---|
| History | Atrial fibrillation (A-fib), atherosclerosis, polyarteritis nodosa |
| Symptoms | Sudden onset abdominal pain (10/10), nausea, vomiting |
| Diagnosis | Acute Mesenteric Ischemia: Confirmed by angiography, followed by laparotomy and resection of the gut |
7. Diverticulitis
| Patient Details | 50-year-old male with rectal bleeding and altered bowel movements |
|---|---|
| Diagnosis | Diverticulitis |
| Laboratory/Imaging | TLC (Total Leukocyte Count) very elevated, CT abdomen |
| Treatment | Surgery |

8. Heyde Syndrome:
A rare condition where aortic stenosis is associated with angiodysplasia, leading to gastrointestinal bleeding.
- Aortic Stenosis is a condition where the aortic valve narrows, restricting blood flow from the left ventricle to the aorta.
- Cough Acquired: Cough caused by various conditions, such as respiratory infections or underlying diseases like aortic stenosis or angiodysplasia.
- Angiodysplasia: Abnormal blood vessels in the gastrointestinal tract, often leading to bleeding, commonly found in Heyde Syndrome.
Here are other materials for NLE NRE step 1
9. Colonic Polyps and Associated Syndromes
| Condition | Details |
|---|---|
| Colonic Polyp | Abnormal growth in the colon, can be benign or precancerous. |
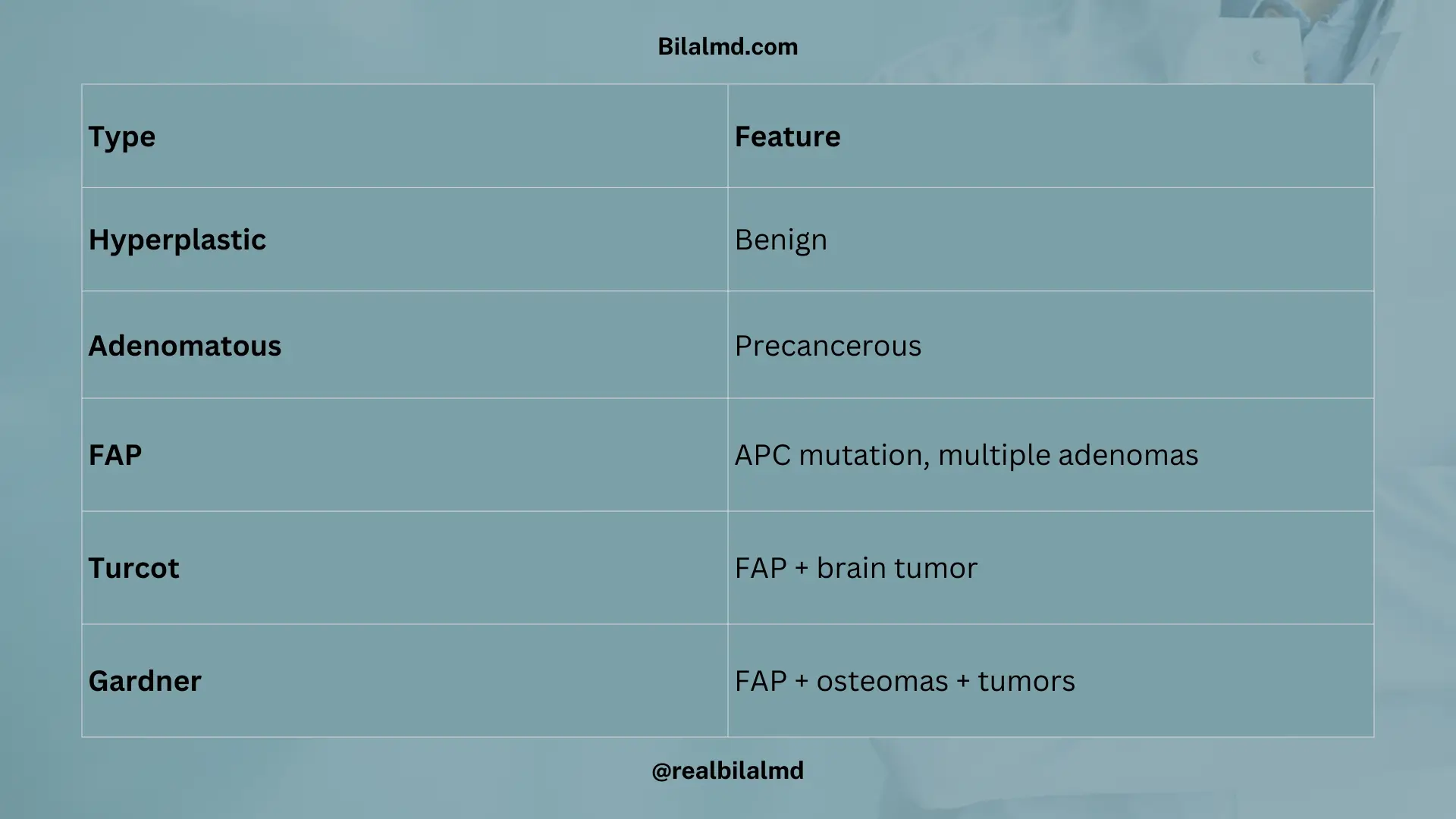
| Hyperplastic Polyp | Benign polyp, typically not associated with cancer risk. |
| Adenomatous Polyp | Can become cancerous, precancerous lesions in the colon. |
| Familial Adenomatous Polyposis (FAP) | Genetic condition associated with numerous adenomatous polyps. Involves mutation of APC gene on chromosome 5. |
| Turcot Syndrome | FAP + Osteoma, a condition that includes colon polyps and bone tumors. |
| Gardner Syndrome | FAP + Brain tumor (often medulloblastoma), along with other features like osteomas and soft tissue tumors. |
10. Colon Cancer
| Condition | Details |
|---|---|
| Risk Factors | Chronic smoking, positive family history, APC gene mutation, low fiber diet. |
| Symptoms/Signs | Older patient, smoker, iron deficiency anemia (rule out colon cancer). |
| Right ascending colon: Exophytic masses, Iron deficiency anemia. | |
| Left descending colon: Infiltrative obstruction. | |
| Tumor Markers | CEA (Carcinoembryonic Antigen): Elevated in recurrence. |
| Diagnosis | Colonoscopy and biopsy for confirmation. |
| Treatment (Tx) | Surgical resection, chemotherapy (if necessary). |
| Recurrence Monitoring | Regular follow-up with CEA levels. |

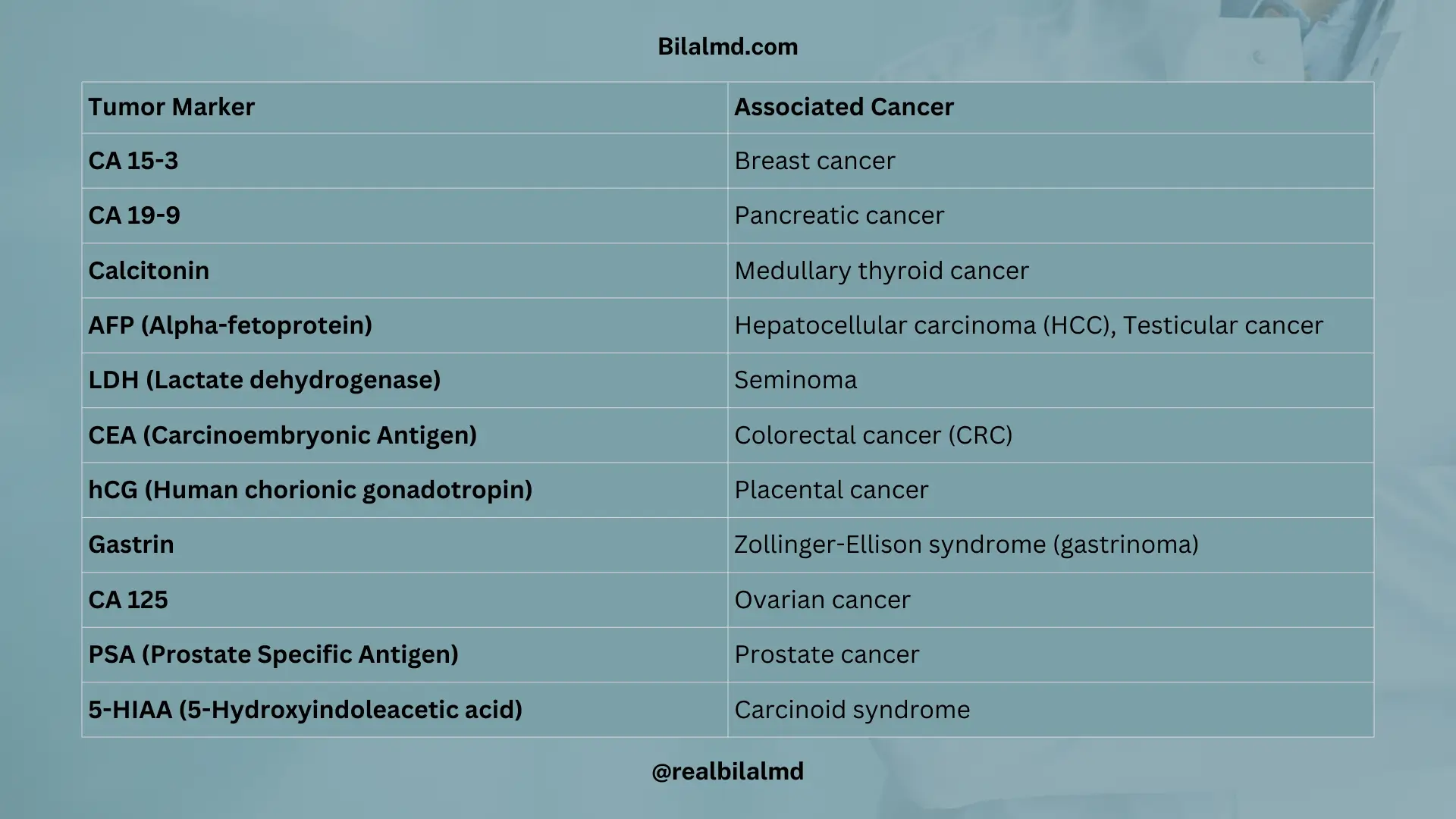
11. Tumor Markers and Associated Cancers
| Tumor Marker | Associated Cancer |
|---|---|
| CA 15-3 | Breast cancer |
| CA 19-9 | Pancreatic cancer |
| Calcitonin | Medullary cancer of the thyroid |
| AFP (Alpha-fetoprotein) | Hepatocellular carcinoma (HCC), testicular cancer |
| LDH (Lactate dehydrogenase) | Seminoma |
| CEA (Carcinoembryonic Antigen) | Colorectal cancer (CRC), |
| hCG (Human chorionic gonadotropin) | Placental cancer |
| Gastrin | Zollinger-Ellison syndrome (gastrinoma) |
| CA 125 | Ovarian cancer |
| PSA (Prostate Specific Antigen) | Prostate cancer |
| 5-HIAA (5-Hydroxyindoleacetic acid) | Carcinoid syndrome |
12. Hepatobiliary Pathologies: Gallstones
| Aspect | Details |
|---|---|
| Risk Factors | 4 F’s: Female, Forty (in age), Fatty, Fertile |
| Gender Prevalence | Female > Male |
| Most Common Type | Cholesterol Stones (90% of cases) |
| Other Type | Pigmented Stones (10%, associated with bile components) |
13. Cholecystitis
| Symptom/Sign | Details |
|---|---|
| Pain | Right upper quadrant pain after eating fatty foods |
| Associated Symptoms | Fever, nausea, tenderness |
| Diagnosis | Negative ultrasound for gallstones (in some cases, not visible) |
| Types of Cholecystitis | Calculous: Presence of gallstones (calculi). |
| Acalculous: No gallstones present, but inflammation exists. | |
| Lab Findings | Blood count (CBC) may show elevated white blood cells (leukocytosis). |
| Imaging | Ultrasound (USG) is the preferred diagnostic tool. |
| Treatment (Tx) | Cholecystectomy (surgical removal of the gallbladder). |

14. Hepatobiliary Pathologies
| Condition | Details |
|---|---|
| Cholelithiasis | Stone formation in the gallbladder. |
| Cholecystitis | Inflammation of the gallbladder, commonly due to E. coli infection. |
| Choledocholithiasis | Stone trapped in the common bile duct (CBD). |
| Cholangitis | Inflammation of the CBD, often presenting with Charcot’s Triad: fever, RUQ pain, and jaundice. |
| Charcot’s Triad | Fever, Right Upper Quadrant (RUQ) pain, and jaundice. |
| Reynold’s Triad | Charcot’s Triad + mental status changes and shock. |
| Diagnosis & Treatment | ERCP (Endoscopic Retrograde Cholangiopancreatography) is used for diagnosis and treatment. |
| Atrophied and fibrotic gallbladder can lead to cancer development. | An atrophied and fibrotic gallbladder can lead to cancer development. |
15. Pancreatic Pathology
| Symptom/Sign | Phase/Category | Potential Diagnosis/Explanation |
|---|---|---|
| Very Intense Pain (10/10) | Acute Phase | Acute Pancreatitis |
| Vomiting | Acute Phase | Acute Pancreatitis |
| Sweating | Acute Phase | Acute Pancreatitis |
| Elevated Serum Amylase and Lipase | Acute Phase | Acute Pancreatitis |
| Recurrent Pain | Chronic Phase | Chronic Pancreatitis |
| Mild Pain | Chronic Phase | Chronic Pancreatitis |
| Steatorrhea | Chronic Phase | Chronic Pancreatitis |
| Maldigestion | Chronic Phase | Chronic Pancreatitis / Pancreatic Insufficiency |
| Normal Amylase and Lipase | Chronic Phase | Chronic Pancreatitis / Pancreatic Insufficiency |
| Weight Loss | Chronic Phase | Chronic Pancreatitis |
| Aspect | Details |
|---|---|
| Hx (History) | Acute Pancreatitis |
| P/C (Presenting Complaints) | Epigastric pain with mass |
| Possible Diagnoses | Pancreatic Pseudocyst, Pancreatic Cyst |
| Associated Lab Findings | Elevated CA 19-9 |
| From Head of Pancreas | Jaundice |
| Physical Exam | Palpable Gallbladder, Courvoisier’s Sign (suggesting obstructive jaundice) |
| Necrosis Type | Associated Condition | Description |
|---|---|---|
| Autodigestion Necrosis | Pancreatitis | Occurs in acute pancreatitis, where pancreatic enzymes digest the tissue of the pancreas itself, leading to necrosis. |
| Liquefactive Necrosis | Pancreatitis | A type of necrosis where the tissue becomes liquefied, commonly seen in acute pancreatitis due to enzyme activity. |
| Fat Necrosis | Trauma / Pancreatitis | Fat cells are broken down into fatty acids and glycerol, often seen in trauma to the pancreas or in pancreatitis. Fatty tissue in the pancreas undergoes necrosis, often with surrounding inflammation. |
16. Anal Fissure
Longitudinal tearing of the anal mucosa.
Risk Factors (R/F):
- Constipation
- Decreased fiber diet
- Obesity
Clinical Features:
- Intense pain in the anal region with defecation.
- Pain persists after defecation.
- Streak of blood in the stool.
Investigation:
- Clinical Diagnosis: Based on presenting symptoms and physical examination.
Management (Tx):
- Diet Changes: Increase fiber intake to prevent constipation.
- Medications:
- Analgesics: Pain relief medications.
- Nitroglycerin: Topical treatment to relax the anal sphincter.

17. Anal Abscess (Complication)
Indications to Consider:
- Throbbing anal pain during defecation.
- High fever, chills, and rigors.
Physical Examination (O/E):
- Tender abdomen.
Management:
- Incision and Drainage (I&D): Surgical procedure to drain the abscess and relieve symptoms.

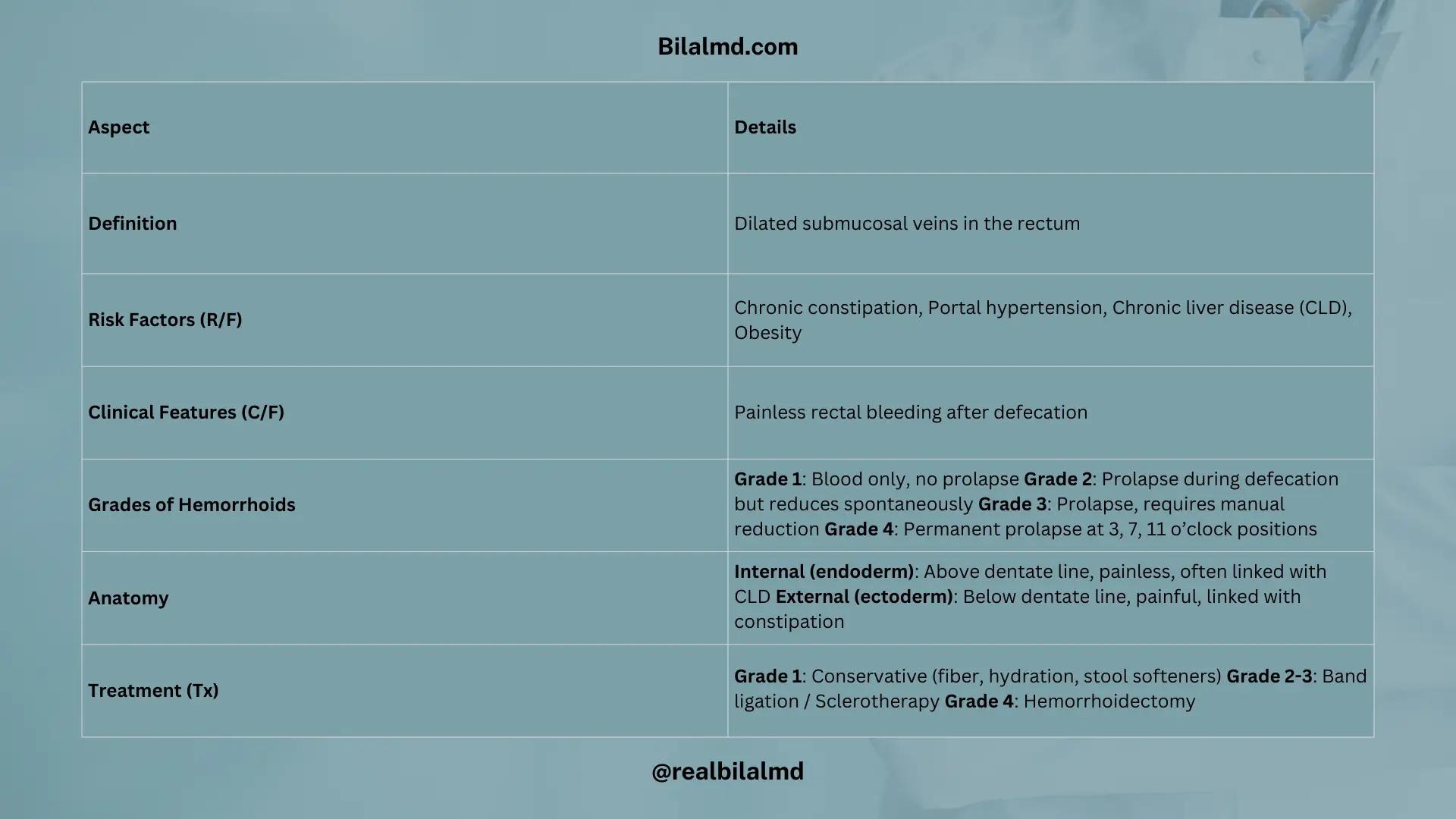
18. Hemorrhoids
Dilated submucosal veins in the rectum.
Risk Factors (R/F):
- Chronic constipation
- Portal hypertension
- Chronic liver disease (CLD)
- Obesity
Clinical Features (C/F):
- Painless PR (per rectum) bleeding: Passage of a drop of blood on feces, usually seen after defecation.
- Type of Hemorrhoids:
- Grade 1: Only blood (no prolapse).
- Grade 2: Mass in and out (prolapses during defecation but reduces spontaneously).
- Grade 3: Manual mass in (prolapses and needs manual reduction).
- Grade 4: Permanent out at 3, 7, 11 o’clock positions (prolapsed and cannot be reduced).
- Anatomy:
- Endoderm (internal hemorrhoids): Painless, associated with chronic liver disease (CLD), and located above the dentate line.
- Ectoderm (external hemorrhoids): Painful, associated with constipation, and located below the dentate line.
Treatment (Tx):
- Grade 1: Conservative: Dietary modifications, increased fiber, stool softeners, and adequate hydration.
- Grade 2, 3: Band ligation (rubber band application to restrict blood flow to the hemorrhoid) or sclerotherapy (injecting a sclerosing agent to shrink the hemorrhoid).
- Grade 4: Hemorrhoidectomy (surgical removal of the hemorrhoid).
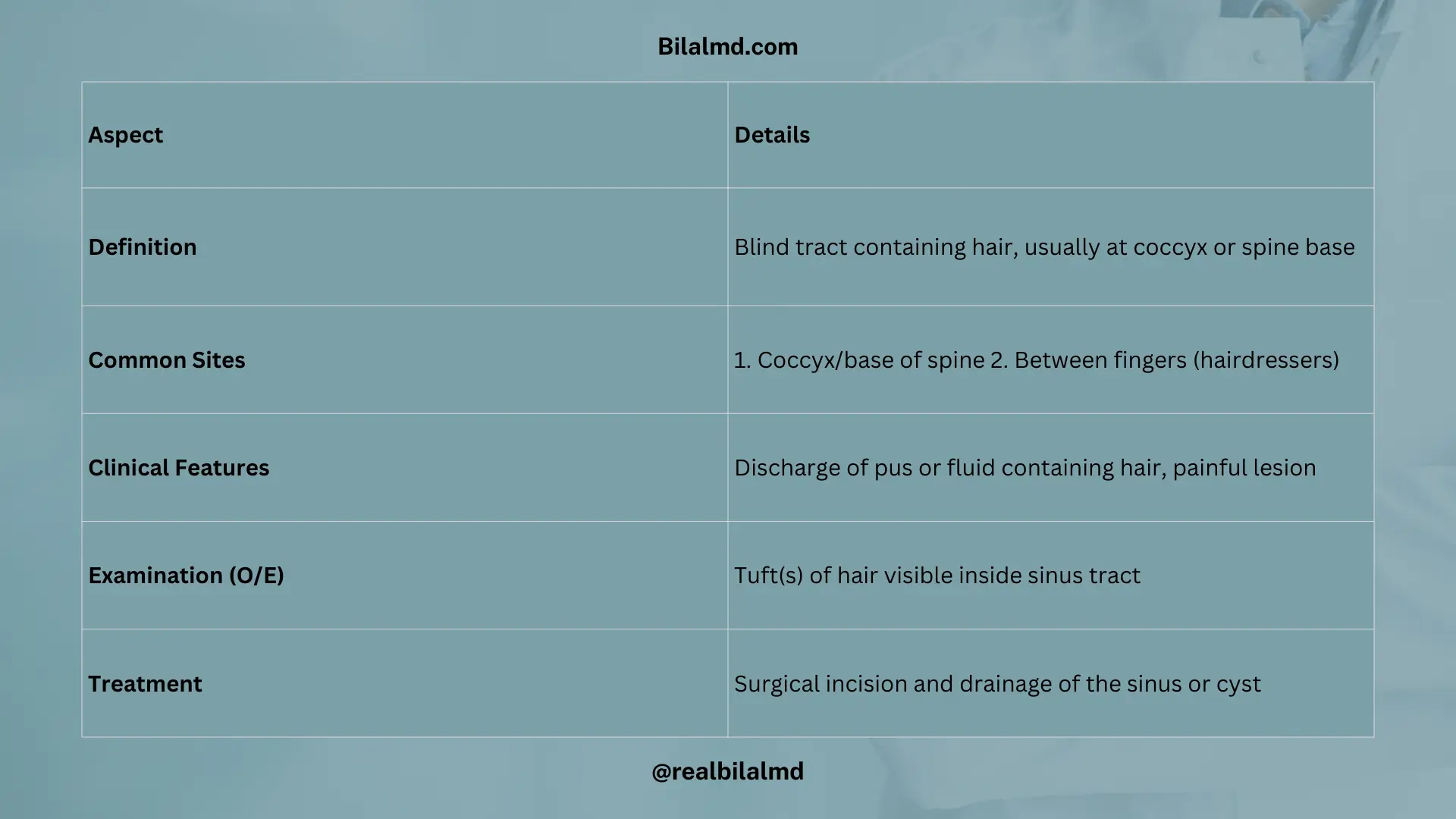
19. Pilonidal Sinus
A connection with a blind tract filled with tuft(s) of hair, often located at the bottom of the spine or coccyx.
Site:
- At the bottom of the spine (near the coccyx).
- At the coccyx.
- Between fingers (often seen in hairdressers).
Clinical Features (C/F):
- Lesion can discharge fluid or pus, often containing hair.
Physical Examination (O/E):
- Presence of tuft(s) of hair in the lesion.
Treatment (Tx):
Surgical Incision: To drain and remove the pilonidal sinus or cyst.
20. Perianal Fistula (Differential Diagnosis)
Hint:
- Middle-aged males may present with persistent pain and discharge in the anal region, peri-anal pruritus, and frequency of wet clothes due to discharge.
- External opening near the anal canal is a key sign.
MRI:
- MRI can be helpful in evaluating the extent of the fistula tract.
Treatment (Tx):
- Fistulectomy: Surgical removal of the fistula.
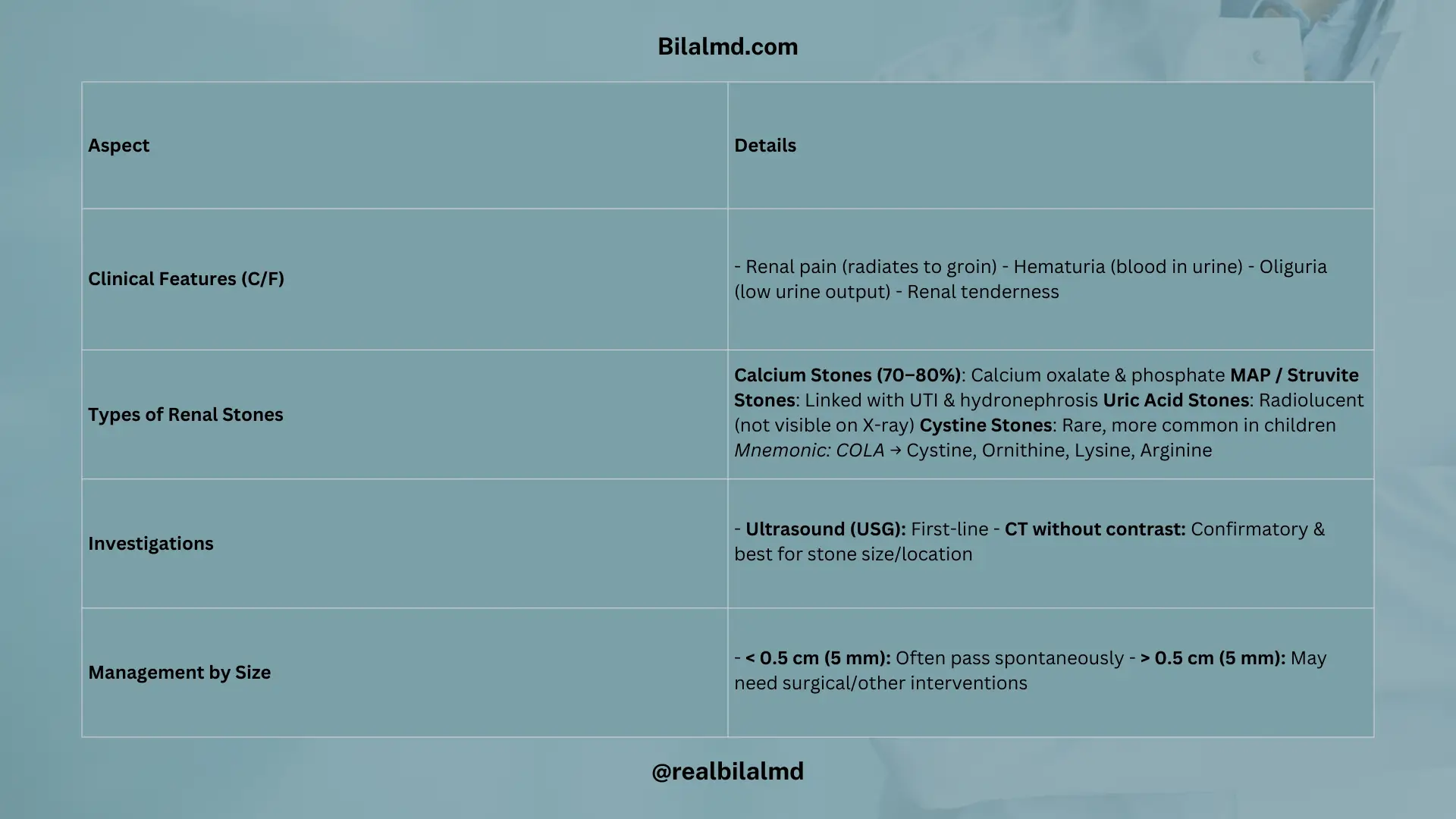
21. Renal Stones
Clinical Features (C/F):
- Renal pain: Often radiates to the groin.
- Hematuria: Blood in the urine, often visible.
- Oliguria: Reduced urine output.
- Renal tenderness: Pain on palpation of the kidney area.
Types of Renal Stones:
- Calcium Stones (70-80%):
- Composed of calcium phosphate and calcium oxalate.
- Magnesium Ammonium Phosphate (MAP) Stones (Struvite Stones):
- Associated with urinary tract infections and hydronephrosis; second most common.
- Uric Acid Stones:
- Radiolucent (do not appear on X-rays).
- Cystine Stones:
- Rare, but common in children.
- Mnemonic for cystine stones: “COLA”
- C – Cystine (hexagonal shape).
- O – Ornithine.
- L – Lysine.
- A – Arginine.
Diagnostic Investigations:
- Ultrasound (USG): Initial imaging tool.
- CT without contrast: A Confirmatory test to diagnose renal stones and determine their size.
Stone Size and Management:
- Size < 0.5 cm (5mm): Stones may pass spontaneously.
- Size > 0.5 cm (5mm): Surgical intervention or other procedures required for removal.
Check your NRE Step 1 result after completing the exam.
Thanks for helping FMGs! Your work is really helpful for students preparing for exams. Keep up the good work😊
Thanks for motivating me to do stuff like that.