1. Menstrual Cycle
A regular monthly physiological cycle in females that increases the chances of pregnancy.
1. Phases of Menstrual cycle
There are 3 phases in the menstrual cycle, and to remember them, use the mnemonic
FOL: Follicular, Ovulatory, and Luteal.
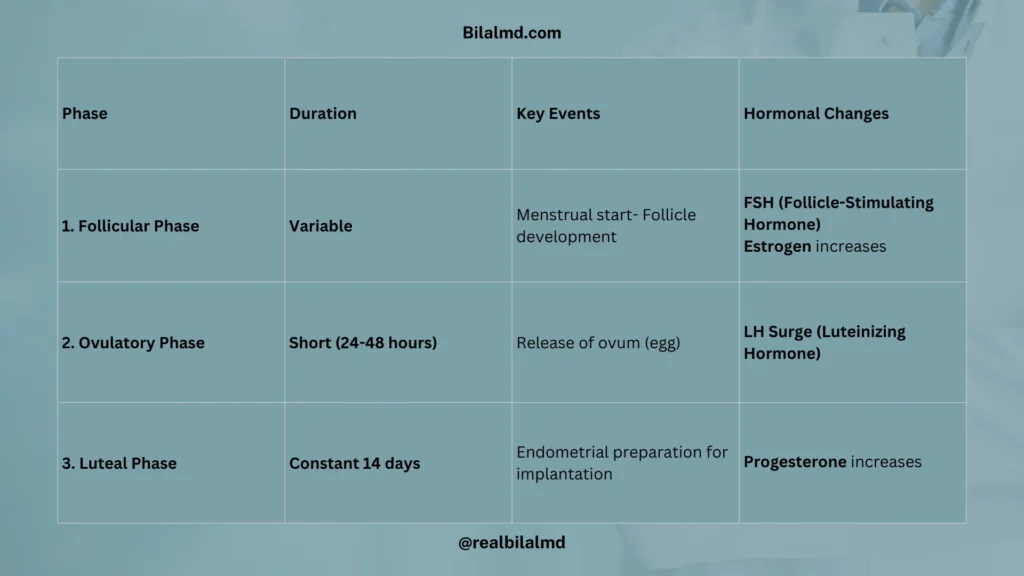
| Phase | Duration | Key Events | Hormonal Changes |
|---|---|---|---|
| 1. Follicular Phase | Variable | Menstrual start- Follicle development | FSH (Follicle-Stimulating Hormone) Estrogen increases |
| 2. Ovulatory Phase | Short (24-48 hours) | Release of ovum (egg) | LH Surge (Luteinizing Hormone) |
| 3. Luteal Phase | Constant 14 days | Endometrial preparation for implantation | Progesterone increases |
The Graafian follicle becomes the ovum under the influence of LH (Luteinizing Hormone), and the corpus luteum then secretes progesterone to support pregnancy.
- FSH (Follicle-Stimulating Hormone), a gonadotropin, acts on the ovary to convert the primary follicle into a secondary follicle.
- LH (Luteinizing Hormone) triggers the ovary to release the ovum (egg).
- After ovulation, the corpus luteum secretes progesterone, which thickens the uterine lining to prepare for pregnancy.
2. Amenorrhea – lack of menses
| Type | Characteristics | Associated Conditions | Diagnosis/Tests |
|---|---|---|---|
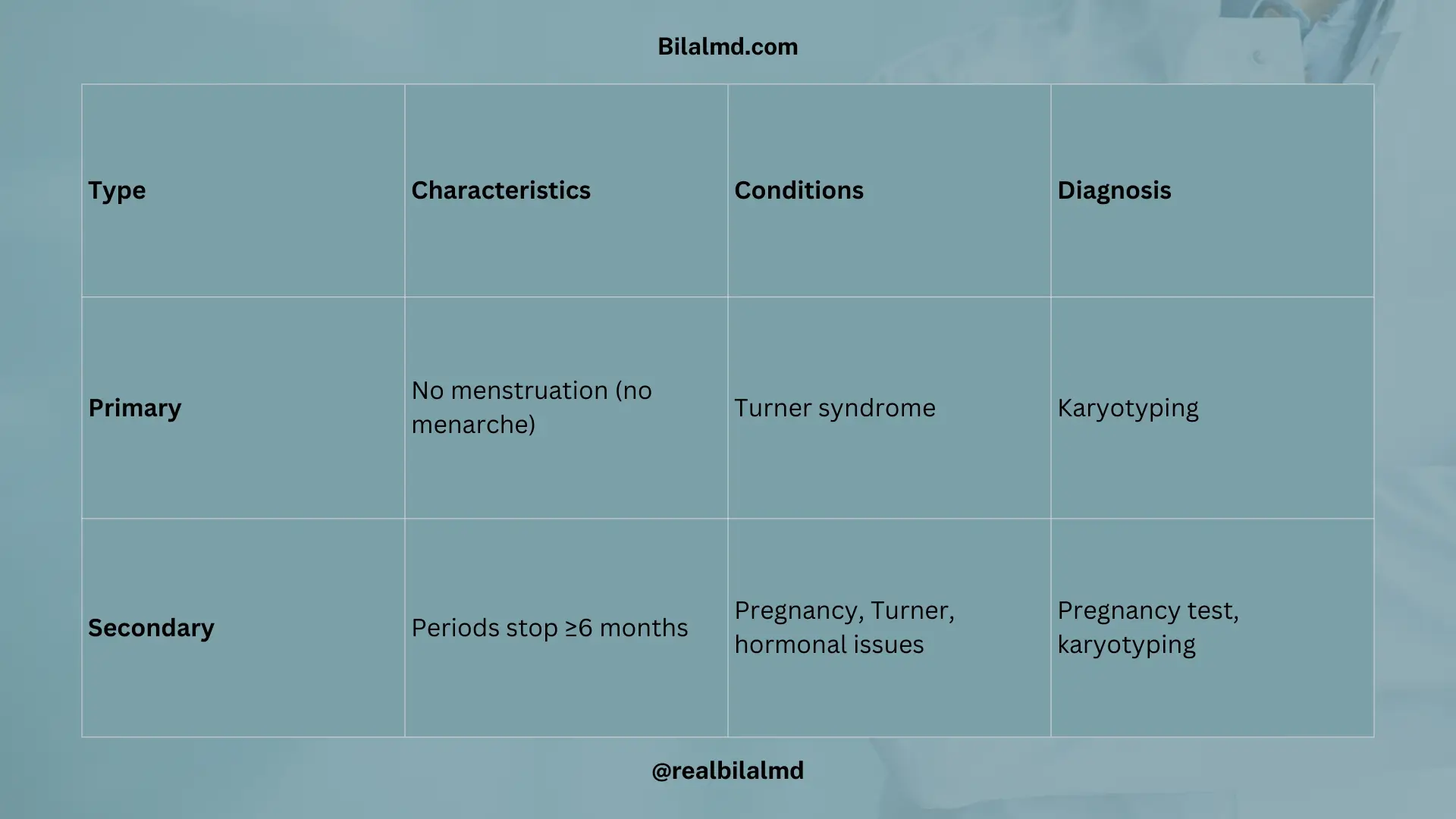
| Primary Amenorrhea | – Lack of menstruation.- Failure to pass menarche (first period). | – Turner Syndrome (may present as primary amenorrhea) | – Karyotyping (to check for chromosomal abnormalities) |
| Secondary Amenorrhea | – Menstruation has occurred but stops for 6 months or more. | – Pregnancy (must be ruled out)- Turner Syndrome (due to streak ovaries)- Other hormonal imbalances | – Pregnancy test- Karyotyping (typically 45,X) |
1. Differential Diagnosis of Amenorrhea
| Possible Diagnosis | Symptoms | Key Findings | Treatment/Management |
|---|---|---|---|
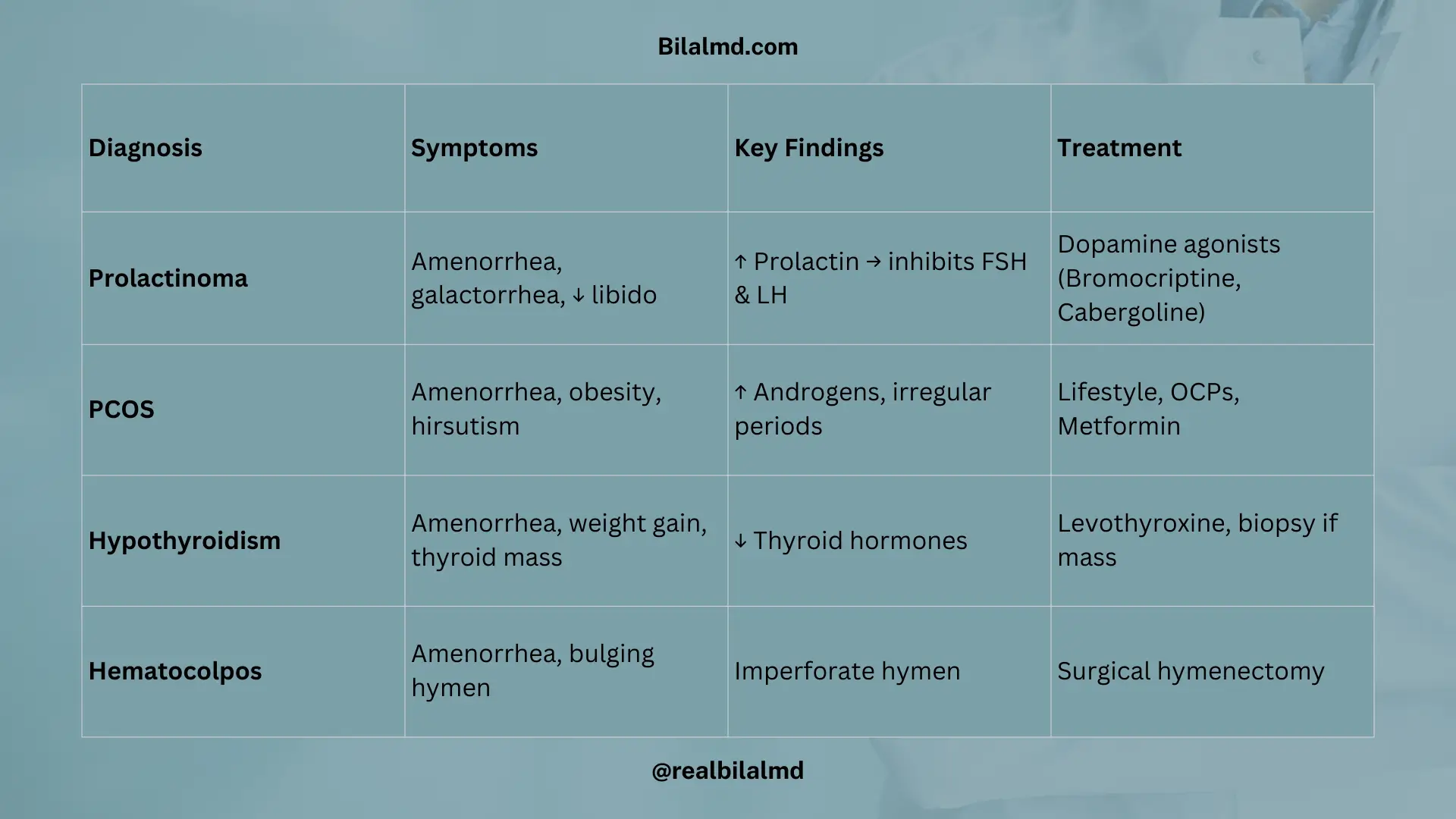
| Prolactinoma | Amenorrhea + Loss of libido + Galactorrhea | Prolactin levels increase.- Inhibits FSH and LH. | Dopamine agonists (e.g., Bromocriptine, Cabergoline) to reduce prolactin levels. |
| PCOS (Polycystic Ovary Syndrome) | Amenorrhea + Obesity + Hirsutism | Irregular periods.- Increased androgens leading to hair growth. | Lifestyle changes (diet/exercise).- Metformin or oral contraceptives for symptom management. |
| Hypothyroidism or Thyroid Disorder | Amenorrhea + Weight gain + Dizziness + Thyroid mass | Low thyroid function.- Possible thyroid nodule or mass. | Thyroid hormone replacement (e.g., Levothyroxine).- Further workup for thyroid mass (e.g., biopsy). |
| Hematocele or Hematocolpos | Amenorrhea + Bulging of vaginal canal (imperforate hymen) | Imperforate hymen leading to blood accumulation in the vaginal canal. | Surgical correction to remove the hymen and allow proper menstrual flow. |
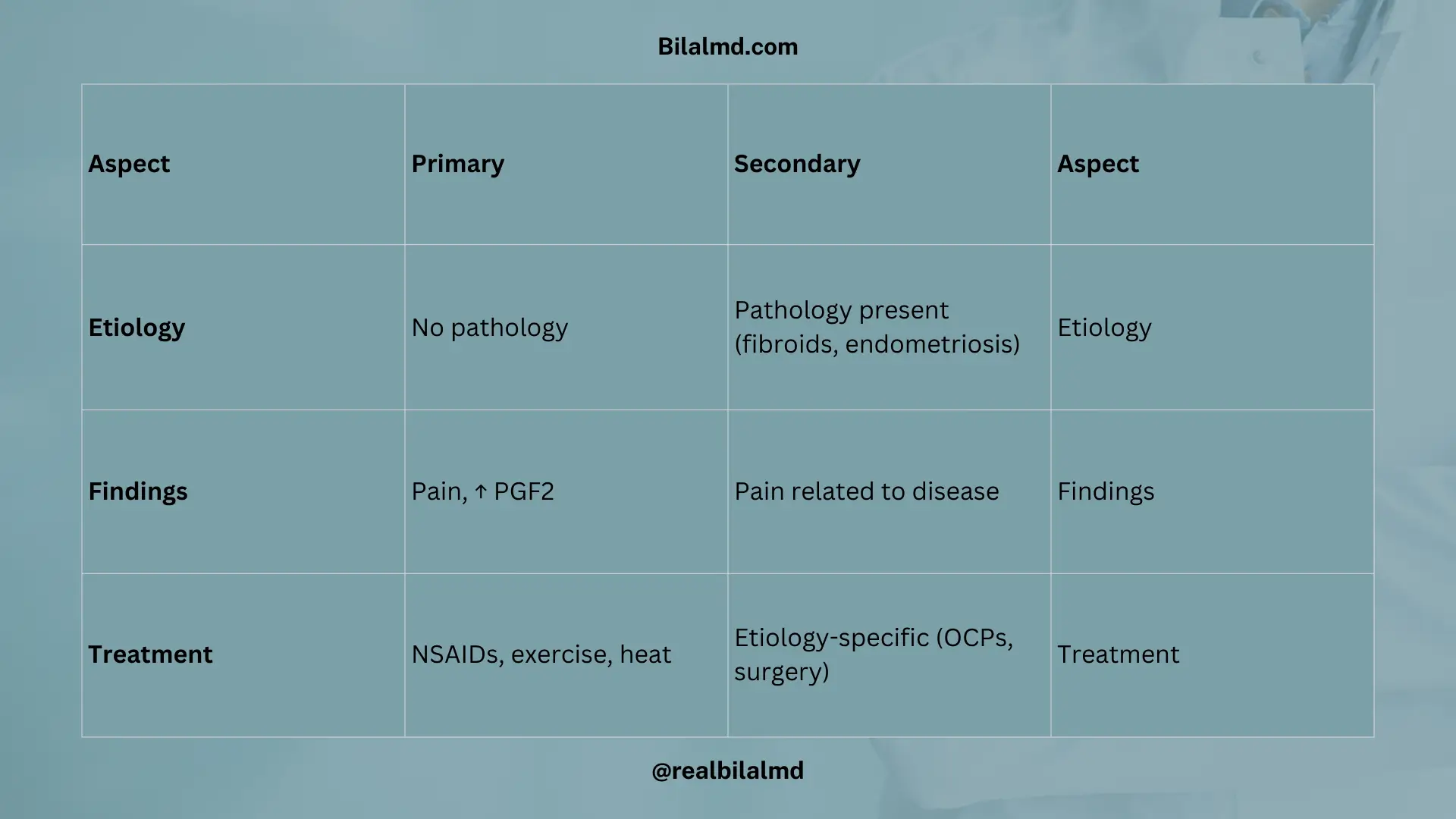
3. Dysmenorrhea: Pain during menstruation
| Aspect | Primary Dysmenorrhea | Secondary Dysmenorrhea |
|---|---|---|
| Etiology | No underlying pathology | Pathology present (e.g., uterine fibroids, endometriosis) |
| Key Findings | – Pain during menstruation- Associated with anoxia– Increased PGF2 (prostaglandin) | – Pain associated with specific pathology- Uterine polyps not typically associated with pain |
| Treatment | – NSAIDs (e.g., Naproxen, Ibuprofen)- Heat therapy– Exercise | – Etiology-specific treatment (e.g., hormonal therapy, surgery, etc., based on the underlying cause) |
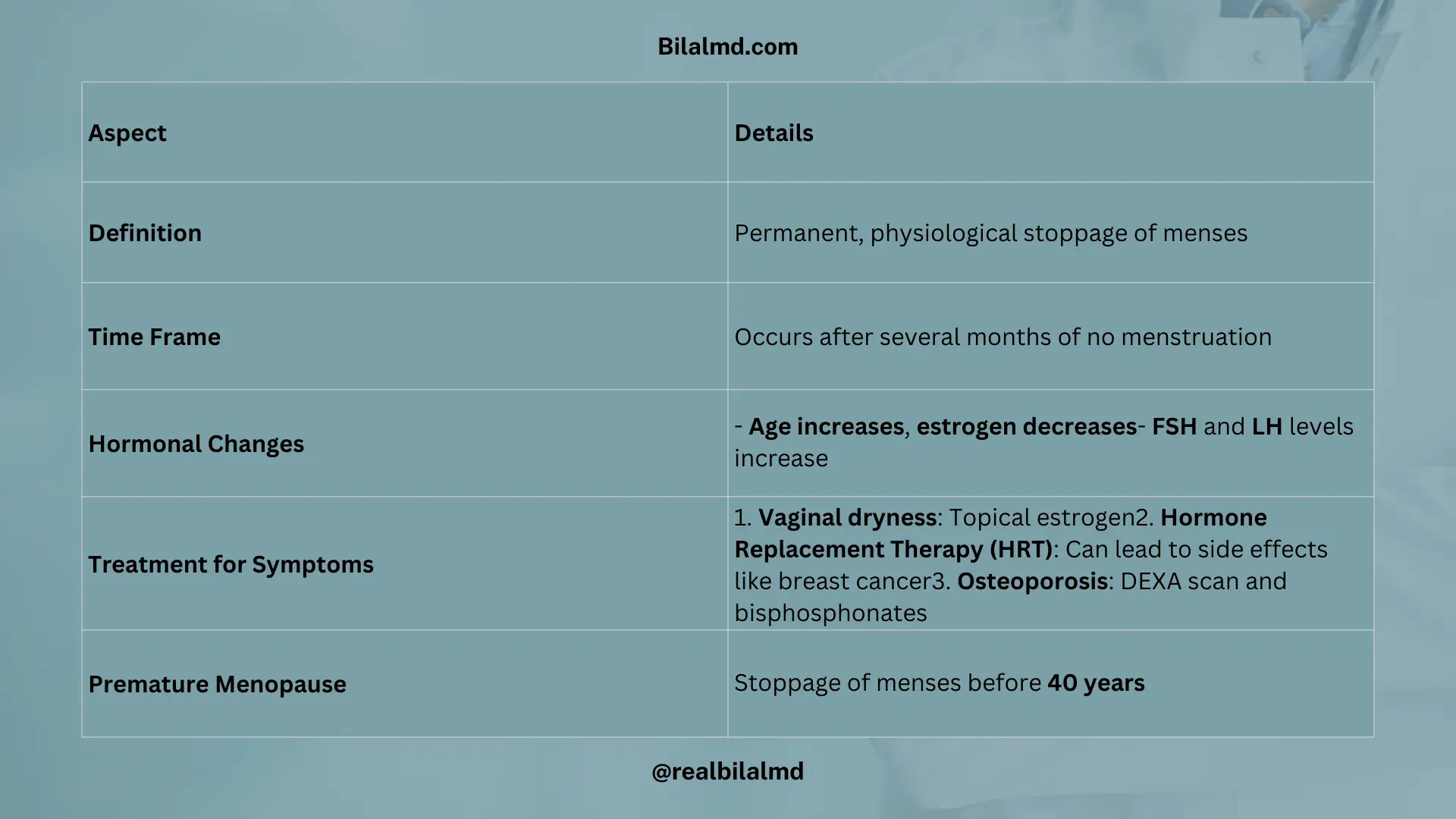
4. Menopause
| Aspect | Details |
|---|---|
| Definition | Permanent, physiological stoppage of menses |
| Time Frame | Occurs after several months of no menstruation |
| Hormonal Changes | – Age increases, estrogen decreases– FSH and LH levels increase |
| Treatment for Symptoms | 1. Vaginal dryness: Topical estrogen2. Hormone Replacement Therapy (HRT): Can lead to side effects like breast cancer3. Osteoporosis: DEXA scan and bisphosphonates |
| Premature Menopause | Stoppage of menses before 40 years |
5. Abnormal/Dysfunctional Uterine Bleeding
There are three parts of the uterus;
| Part of Uterus | Description |
|---|---|
| 1. Perimetrium | Outer serous layer of the uterus; part of the peritoneum. |
| 2. Myometrium | Middle muscular layer; responsible for uterine contractions during labor. |
| 3. Endometrium | Inner mucosal lining; thickens during the menstrual cycle to support embryo implantation. |
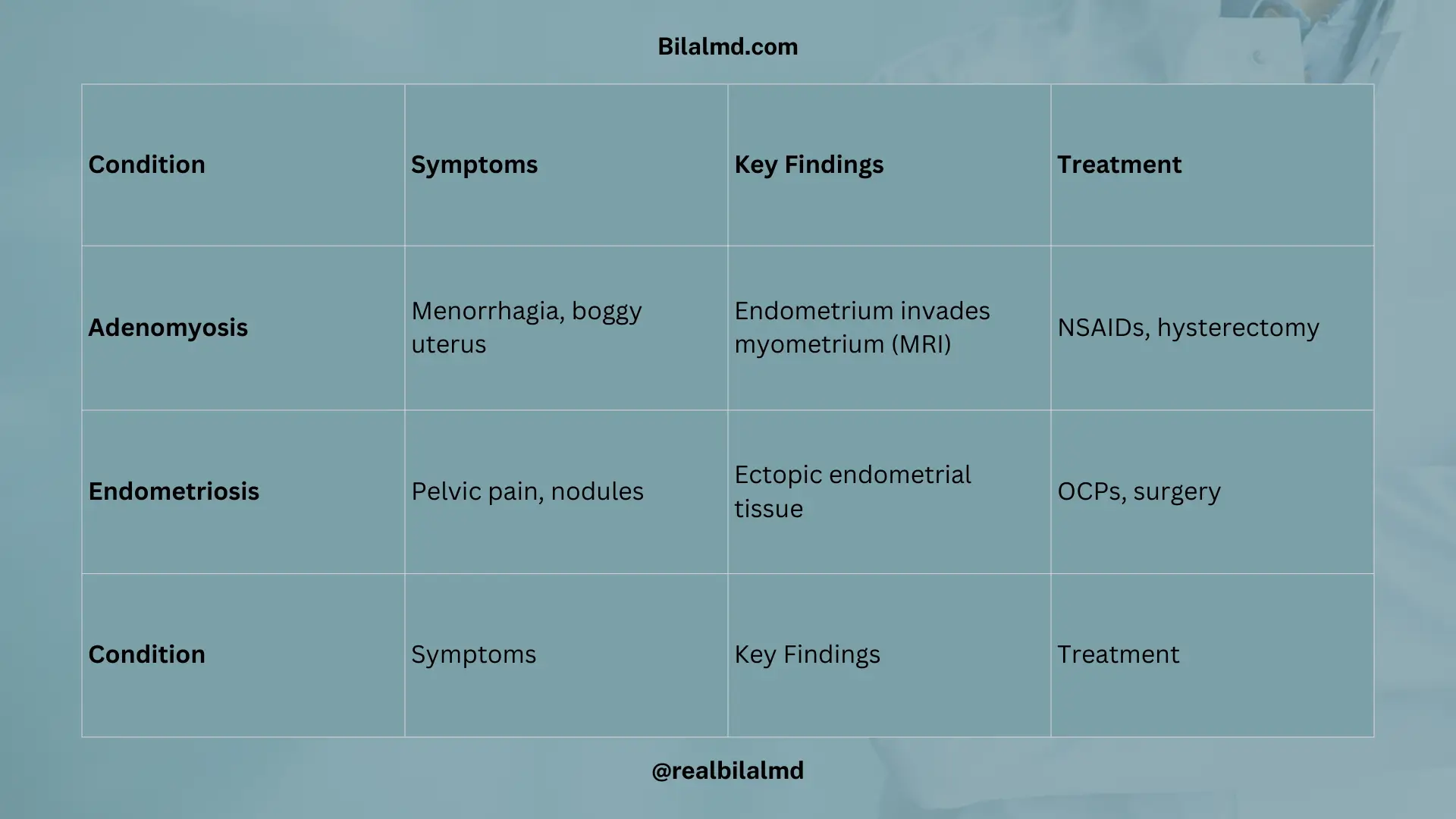
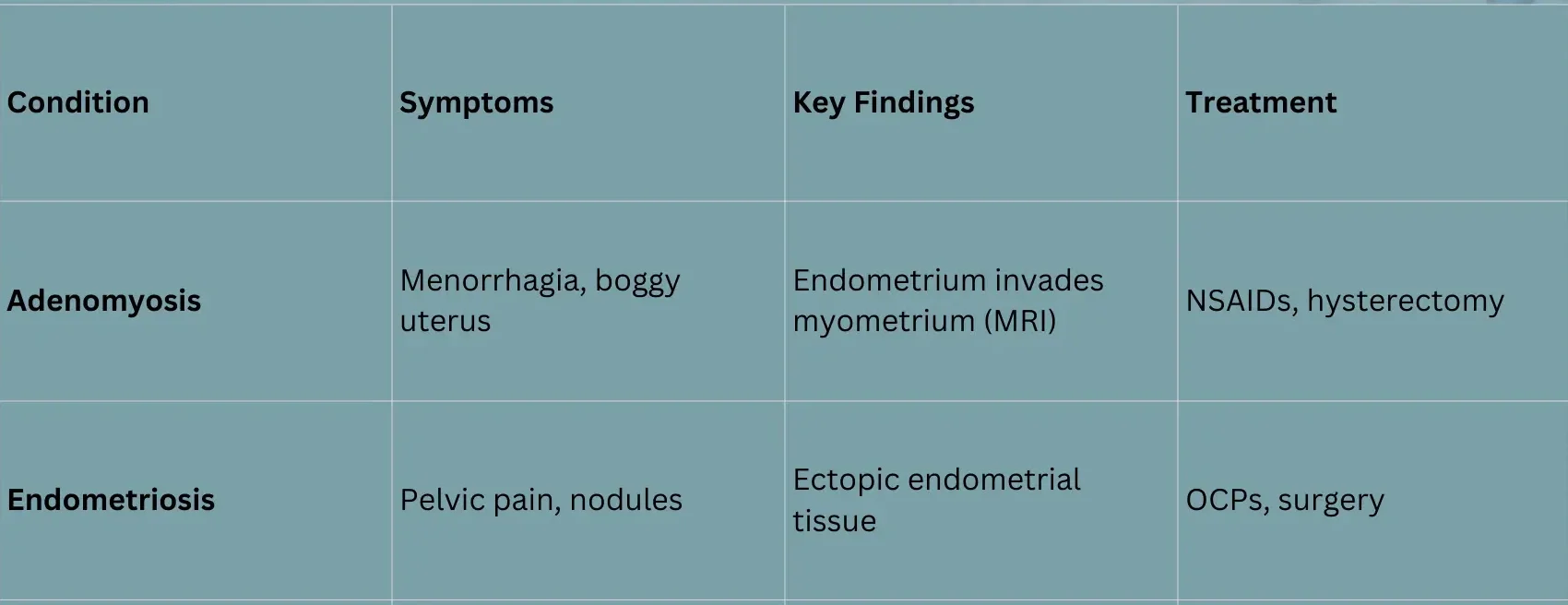
| Aspect | Adenomyosis | Endometriosis |
|---|---|---|
| Symptoms | Pain during menstruation- Menorrhagia (heavy bleeding)- Boggy uterus | – Pelvic pain- Painful nodules in the pelvis- Non-boggy uterus |
| Key Findings | MRI shows tissue from the endometrium invading the myometrium | – MRI shows endometrial tissue covering all layers of the uterus, and can involve abdomen or ovaries (e.g., cysts) |
| Treatment/Management | NSAIDs (for pain relief)- TAH (Total Abdominal Hysterectomy) if severe | – OCPs (Oral Contraceptive Pills)- TAH or Oophorectomy (if ovaries are involved) |
6. PCOS
| Aspect | Details |
|---|---|
| Common Causes of Infertility | PCOS is one of the most common causes of infertility in young females. |
| Symptoms | Young, obese females– Menstrual irregularity– Acne– Hirsutism (excessive hair growth) |
| Ultrasound Findings | Multiple cystic ovaries visible on USG (ultrasound) |
| Lab Findings | LH:FSH ratio increased to 2:1 (LH is higher than FSH) |
| Rotterdam Criteria | Oligomenorrhea (infrequent menstruation)- Hyperandrogenism (elevated male hormones)- Obesity– Cystic ovaries |
1. PCOS Complications
| Aspect | Details |
|---|---|
| Complications | Diabetes (DM)– Acanthosis nigricans (skin darkening, especially around the neck and armpits)- Infertility |
| Ultrasound Findings | Transvaginal USG shows 79-11 cysts in the ovaries.- Necklace appearance (string of pearls appearance on ultrasound). |
| Management (Desire to Conceive) | Metformin (helps with insulin resistance)- Clomiphene (to stimulate ovulation) |
| Management (Do Not Want to Conceive) | Metformin (helps with insulin resistance)- Oral Contraceptive Pills (OCPs) to regulate menstrual cycle and reduce androgens. |
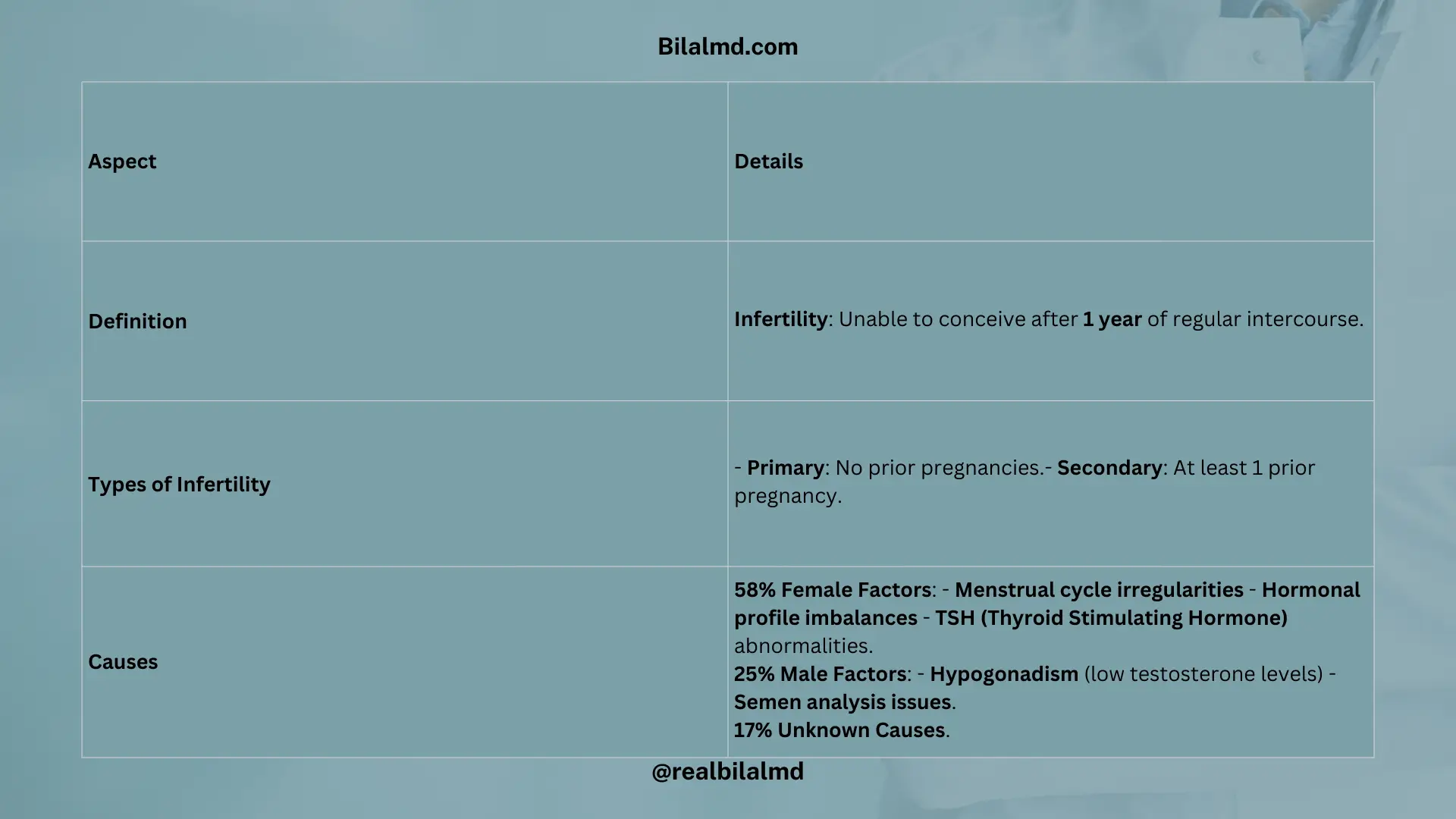
7. Infertility
| Aspect | Details |
|---|---|
| Definition | Infertility: Unable to conceive after 1 year of regular intercourse. |
| Types of Infertility | Primary: No prior pregnancies.- Secondary: At least 1 prior pregnancy. |
| Causes | 58% Female Factors: – Menstrual cycle irregularities – Hormonal profile imbalances – TSH (Thyroid Stimulating Hormone) abnormalities. 25% Male Factors: – Hypogonadism (low testosterone levels) – Semen analysis issues. 17% Unknown Causes. |
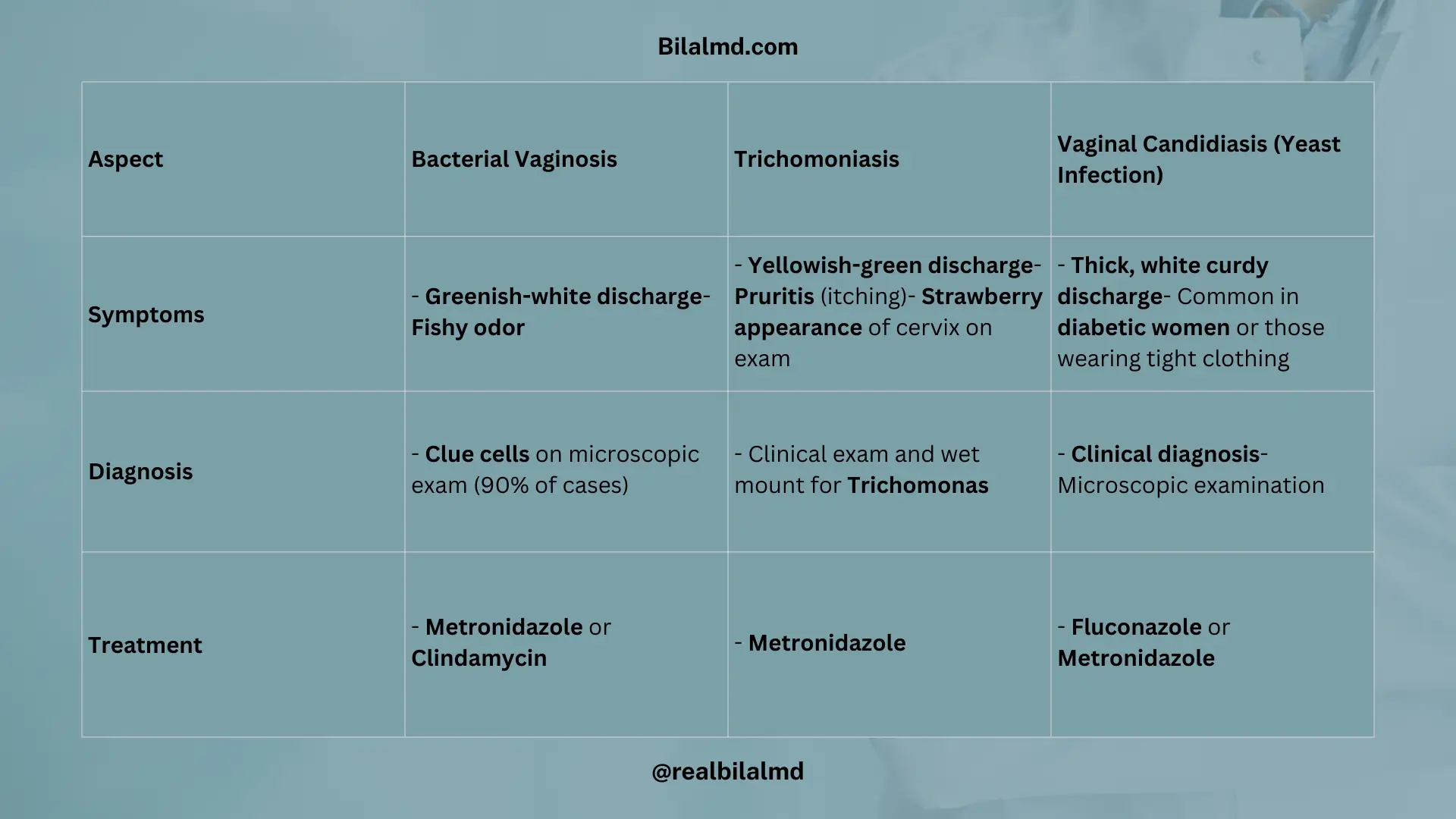
8. Vaginitis
| Aspect | Bacterial Vaginosis | Trichomoniasis | Vaginal Candidiasis (Yeast Infection) |
|---|---|---|---|
| Symptoms | Greenish-white discharge– Fishy odor | Yellowish-green discharge– Pruritis (itching)- Strawberry appearance of cervix on exam | Thick, white curdy discharge– Common in diabetic women or those wearing tight clothing |
| Diagnosis | Clue cells on microscopic exam (90% of cases) | Clinical exam and wet mount for Trichomonas | Clinical diagnosis– Microscopic examination |
| Treatment | Metronidazole or Clindamycin | Metronidazole | Fluconazole or Metronidazole |
9. Toxic Shock Syndrome
| Aspect | Details |
|---|---|
| Cause | Often occurs in individuals using tampons, which provide a medium for bacteria like Staphylococcus aureus (and sometimes Streptococcus). |
| Symptoms/Triad | Fever, Hypotension, Exfoliative dermatitis (peeling skin) |
| Treatment | Broad-spectrum antibiotics to target the bacteria.Supportive care for hypotension (e.g., fluids). |
10. Pelvic inflammatory disease (PID)
| Aspect | Details |
|---|---|
| Affected Areas | 1. Vagina 2. Uterus 3. Fallopian tubes 4. Ovary |
| Symptoms | 1. Pelvic pain 2. Tenderness 3. Vomiting 4. Vaginal discharge |
| Diagnosis | Vaginal swab to look for Neisseria gonorrhea, Chlamydia trichomonas, or other infections |
| Treatment | Broad-spectrum antibiotics to cover a range of pathogens |
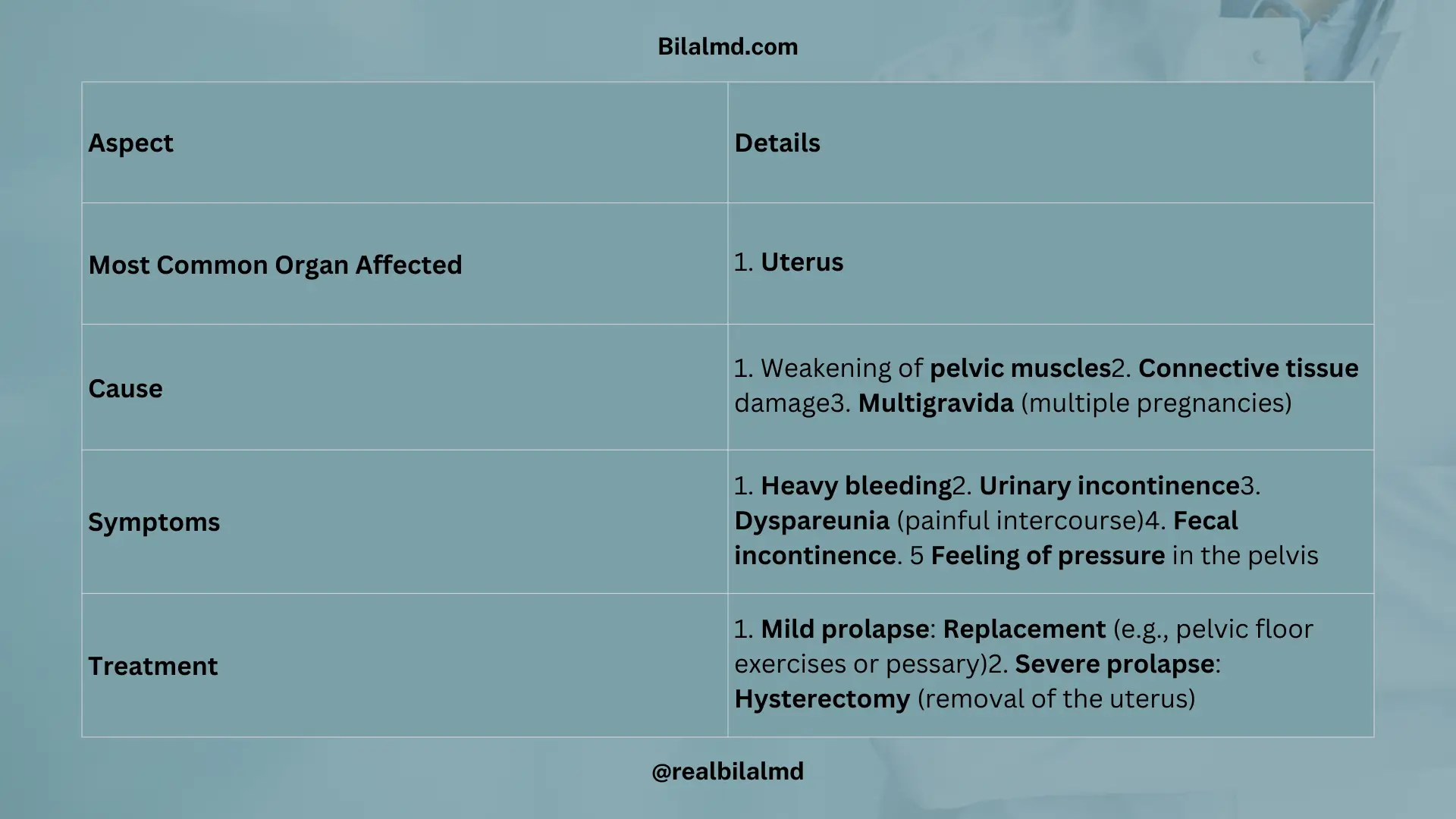
11. Pelvic Organ Prolapse
| Aspect | Details |
|---|---|
| Most Common Organ Affected | 1. Uterus |
| Cause | 1. Weakening of pelvic muscles 2. Connective tissue damage 3. Multigravida (multiple pregnancies) |
| Symptoms | 1. Heavy bleeding 2. Urinary incontinence 3. Dyspareunia (painful intercourse) 4. Fecal incontinence. 5 Feeling of pressure in the pelvis |
| Treatment | 1. Mild prolapse: Replacement (e.g., pelvic floor exercises or pessary) 2. Severe prolapse: Hysterectomy (removal of the uterus) |
12. Urinary Incontinence
| Aspect | Stress Incontinence | Urge Incontinence | Overflow Incontinence |
|---|---|---|---|
| Complaints | Dribbling of urine– Occurs when abdominal pressure increases | Increased sensitivity to the need to pee | Bladder full, but no response to urinate |
| Causes/Triggers | Lifting heavy weights- Chronic constipation- Sneezing- Coughing- Laughter | Overactive bladder- Urge to urinate frequently | Full bladder, but unable to empty it completely |
| Treatment | Kegel exercises to strengthen pelvic floor muscles | Bladder training and medications (e.g., anticholinergics) | Kegel exercises– Catheterization if needed |
13. Conception
| Aspect | Details |
|---|---|
| Conception Prevention | Young females without medical complaints can be recommended OCP (Oral Contraceptive Pills) for contraception. |
| Contraindications for OCP | 1. Liver issues 2. Kidney issues 3. Coagulopathy (blood clotting) disease 4. Migraine headaches (may lead to stroke) 5. History of breast cancer |
| For Breastfeeding | Progesterone-only pills are recommended for breastfeeding women. |
| Middle-aged Female | Long-term contraception can be recommended, such as IUD (Intrauterine Device). |
| Prevent STIs | Use condoms or other barrier methods to prevent sexually transmitted infections (STIs). |
14. Gynecology Cancer
| Aspect | Details |
|---|---|
| Cervical Cancer | Commonly caused by HPV (Human Papillomavirus) infection. |
| Risk Factor | HPV types 16 and 18 are most commonly associated with cervical cancer. |
| Viral Infection | HPV 6 & 11 cause genital warts.- HPV 16 & 18 are linked to cervical cancer. |
| Symptoms | Post-coital bleeding (bleeding after sexual intercourse). |
| Screening Test for Cervical Cancer | Pap smear (used to detect abnormal cells and early signs of cancer). |
| Examination for Post-Coital Bleeding | 1. Trauma (could be due to injury) 2. No trauma (could indicate underlying pathology such as cancer) |
| Diagnostic Procedures | Biopsy for confirmation of cervical cancer.- Pap smear for early detection and screening. |
1. Incidence and Mortality
| Aspect | Details |
|---|---|
| Incidence | Endometrial cancer > Ovarian cancer > Cervical cancer |
| Mortality | Ovarian cancer > Endometrial cancer > Cervical cancer |
| Cervical Biopsy | Taken from the transformation zone (area where the squamous and columnar epithelium meet) |
| Bleeding Causes | Vaginal atrophy (80-90% of cases) |
| Treatment for Vaginal Atrophy | Topical estrogen for management |
| Endometrial Sampling | Well-differentiated (acute): Leads to TAH (Total Abdominal Hysterectomy)- Poorly differentiated: May lead to metastasis and requires chemotherapy and radiation along with TAH |
2. Endometrial Cancer
| Aspect | Endometrial Cancer | Serous Carcinoma (Endometrial Cancer) |
|---|---|---|
| Type | Endometrial Cancer | Serous Carcinoma (a subtype of Endometrial Cancer) |
| Incidence | 75% of uterine cancers | 25% of Endometrial cancer cases |
| Age Range | Typically affects women 55-60 years | Affects women 65-70 years |
| Prognosis | Good prognosis | Poor prognosis due to its aggressive nature |
| Risk Factors | Unopposed estrogen | Associated with genetic mutations and unopposed estrogen |
| Genetic Factor | – | More common in women 65-70 years with genetic mutations |
Adnexal masses, weight loss, and an elevated CA 125 are likely indicative of Ovarian Cancer.
3. Meigs’ Syndrome
- Pleural effusion
- Ascites
- Ovarian tumor
2. OBS
The branch of medicine that focuses on the care of the mother during pregnancy and the fetus.
| Most Common Site of Fertilization | Ampulla of the fallopian tube: The most common site where fertilization occurs. |
| Most Common Site of Implantation | Uterus: The site where the fertilized egg implants and develops into a fetus. |
1. Pregnancy
| Aspect | Details |
|---|---|
| Fetal Period | Starts from 9 weeks of pregnancy |
| Embryogenesis | Occurs from 3 weeks to 8 weeks of pregnancy |
| Cervical Dilation | 10 cm: Full cervical dilation during labor |
2. Stages of labor
| Stage | Description |
|---|---|
| 1st Stage | Uterine contractions leading to cervical dilation. |
| 2nd Stage | From full cervical dilation to the birth of the baby. |
| 3rd Stage | Removal of the placenta after the baby is born. |
3. Hypertensive Disorders in Pregnancy
| Condition | Description |
|---|---|
| Chronic Hypertension | 1. Hypertension develops before 20 weeks of pregnancy. 2. No proteinuria. |
| Gestational Hypertension | 1. Hypertension after 20 weeks of pregnancy. 2. No proteinuria. |
| Preeclampsia | 1. Hypertension after 20 weeks of pregnancy. 2. Proteinuria present. |
| Eclampsia | Preeclampsia with the addition of seizures. |
1. Treatment
- Alpha-methyl dopa
- Labetalol (acts on both alpha and beta receptors)
- Hydralazine for SBP >180 and DBP >110
- Magnesium sulfate (MgSO4) for seizures in Eclampsia
- Calcium gluconate for Magnesium sulfate toxicity
4. HELLP Syndrome:
Remember “HEL” mnemonic
- H: Hemolysis – leading to anemia.
- E: Elevated liver enzymes.
- L: Low platelets.
1. Management:
Emergency C-section delivery is often required, especially after 32 weeks of pregnancy.
5. Ectopic Pregnancy
Implantation of the fertilized egg outside the uterus.
1. Symptoms:
- Amenorrhea (absence of menstruation)
- Lower abdominal pain
- Vaginal spotting
2. Diagnostic Tests:
- Beta-hCG: Elevated but not as high as normal pregnancy levels.
- Transvaginal ultrasound: Empty uterus, indicating the fertilized egg is outside the uterus.
3. Treatment:
Methotrexate: Used to dissolve fetal tissue, as it is a folic acid synthesis inhibitor that stops the growth of cells.
6. TORCH Infections
| Infection | Symptoms/Signs | Treatment |
|---|---|---|
| 1. Toxoplasmosis | 1. Hydrocephalus 2. Intracranial calcifications 3. Chorioretinitis | 1. Pyrimethamine + Sulfadiazine |
| 2. Rubella Virus Infection | 1. Cataracts 2. Patent ductus arteriosus (PDA) 3. Hearing loss 4. Blueberry rashes 5. Mental retardation (MR) | 1. Vaccinate before pregnancy (no specific treatment for congenital rubella) |
| 3. Cytomegalovirus (CMV) | 1. Petechial rashes2. Periventricular calcifications | 1. Ganciclovir |
| 4. Herpes Simplex Virus (HSV) | 1. Skin 2. Eye 3. CNS 4. Oral cavity | 1. Acyclovir |
| 5. Syphilis | 1. Saddle nose 2. Hutchinson 3. Osteitis 4. Hepatomegaly | 1. Penicillin |
7. Abortion
Loss of fetus before the 20th week of pregnancy. Total Body Weight Loss: 500 mg.
Types of Abortion
- Spontaneous Abortion (miscarriage)
- Medically Induced Abortion
| Type of Abortion | Symptoms | Ultrasound Findings |
|---|---|---|
| Incomplete Abortion | Bleeding from vagina- Partial loss of products of conception (POC) | Cervical os open, POC in uterus |
| Inevitable Abortion | Bleeding from vagina | Cervical os open, POC in uterus |
| Complete Abortion | Bleeding from vagina- Abdominal cramps | Cervical os closed, empty uterus |
| Threatened Abortion | Bleeding from uterus- Abdominal pain | Cervical os closed, no POC, fetal cardiac activity present |
| Missed Abortion | No fetal cardiac activity | Cervical os closed, no fetal heartbeat |
Morning sickness: Less than 13 weeks.
Hyperemesis gravidarum: After 13 weeks with dehydration.
Beta-hCG: Increases significantly in twins or mole.
Treatment (TX):
- Pyridoxine (B6)
- IV fluids + Ondansetron
- Metoclopramide
Diagnosis (Dx): Clinical.
Here are other materials for NLE NRE step 1
8. UTI (Urinary Tract Infection):
- Symptoms: Lumbar pain, dysuria (painful urination), hematuria (blood in urine), and fever.
- E. coli: The most common causative organism for UTI.
Diagnosis (Dx):
- Urine R/E (Routine Examination): To check for signs of infection like leukocytes, nitrites, and blood.
- Urine culture: To identify the causative organism and its antibiotic sensitivity.
Treatment (Tx):
- Ceftazidime (Cefta): A broad-spectrum antibiotic commonly used for UTI, particularly when the organism is E. coli.
9. Shoulder Dystocia:
Occurs during birth when the shoulder gets stuck behind the mother’s pelvic bone, leading to a prolonged second stage of labor.
Management:
- McRobert’s maneuver.
- Suprapubic pressure.
- Wood’s screw maneuver.
- Episiotomy
Complications:
- Brachial Plexus Injury.
- Horner’s Syndrome.
10. Preterm Labour
Occurs when labor starts between 10 to 36 weeks of pregnancy.
Common Cause of Neonatal Mortality
It is a leading cause of neonatal death due to complications like respiratory distress syndrome and organ immaturity.
Management:
Hydration & Bed Rest: Aims to reduce contractions and promote fetal well-being.
Tocolytic Therapy:
- Beta-2 Agonists (e.g., Terbutaline): To relax the uterus and delay labor.
- Calcium Channel Blockers (e.g., Nifedipine): Used to prevent uterine contractions.
- Magnesium Sulfate (MgSO4): For uterine relaxation and fetal neuroprotection if the pregnancy is very preterm.
- Betamethasone: A corticosteroid to enhance fetal lung maturity and reduce respiratory issues.
- Prostaglandins: Used in some cases to help induce labor or soften the cervix.
- Penicillin: Administered to prevent Group B Streptococcus (GBS) infection.
11. Fetal Malpresentation
Any position other than the head-first (vertex) presentation.
Breech Position
The fetal buttocks or feet are positioned to come out first during labor.
- Frank Breech:
- Thighs are flexed, and knees are extended.
- Footling Breech:
- One or both legs are extended.
- Complete Breech:
- Both thighs and knees are flexed.
1. Management (Tx):
C-section: Typically the preferred method for breech deliveries to prevent complications.
2. Indications for C-section:
- Previous C-section History: If there’s a history of a previous C-section, a repeat cesarean might be recommended.
- HIV: To reduce the risk of transmission to the baby.
- Adverse Conditions: Such as HPV, cancer, or other contraindications for vaginal birth.
- Decreased Heart Rate: Suggesting fetal distress during descent.
- Fetal Demise: If the fetus has died in utero.
- Umbilical Cord Distress: If the cord is compressed, affecting fetal oxygenation.
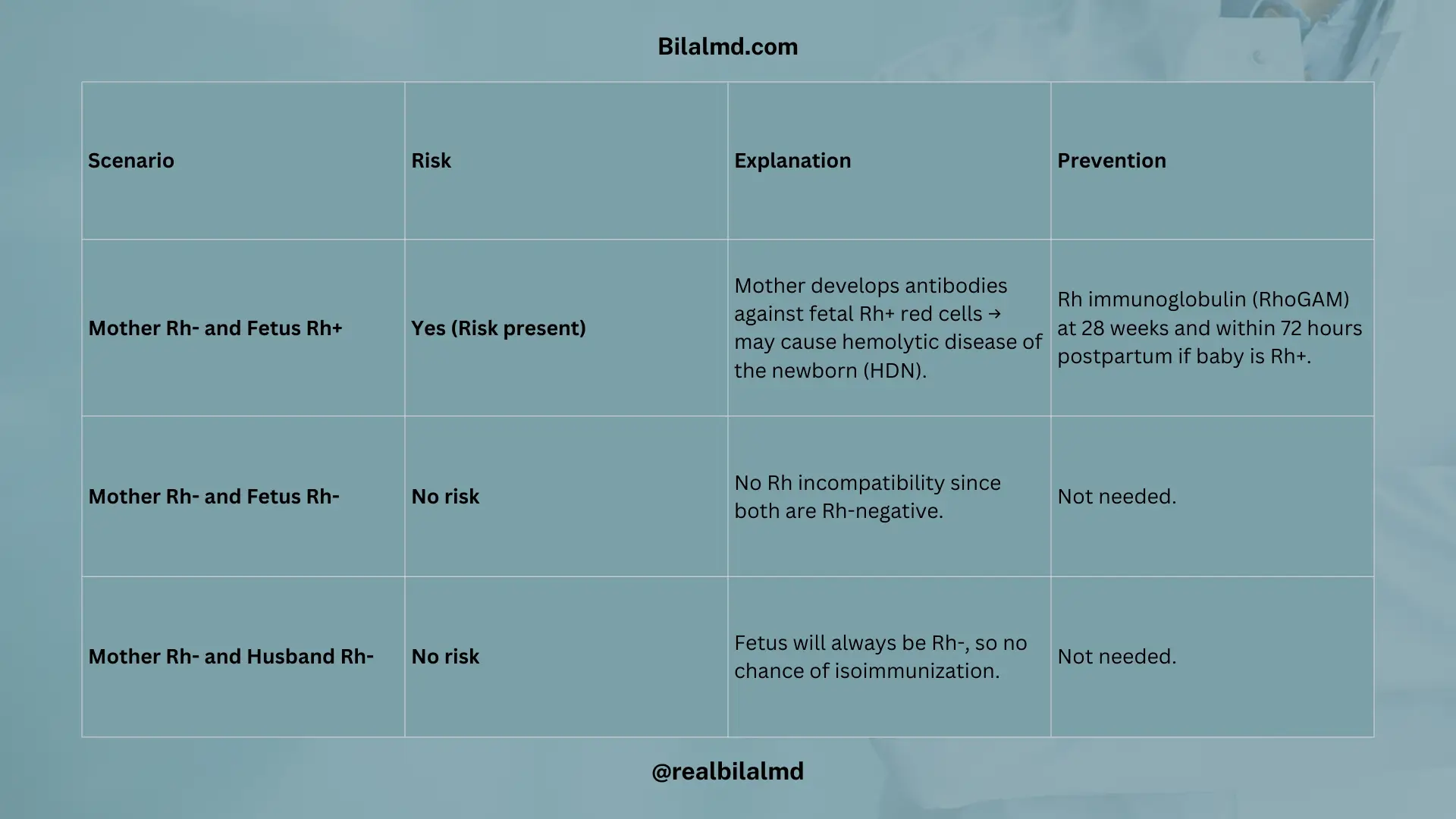
12. Rh Isoimmunization
Occurs when an Rh-negative mother produces antibodies against Rh-positive fetal red blood cells.
Scenarios:
1. Mother Rh- and Fetus Rh+
Risk: Rh incompatibility may lead to the mother’s immune system attacking the fetus’s red blood cells, causing hemolytic disease of the newborn (HDN).
Prevention: Rh immunoglobulin (RhoGAM) is given to the mother to prevent the formation of antibodies.
2. Mother Rh- and Fetus Rh-
No risk: There is no Rh incompatibility as both the mother and fetus are Rh-negative, so no antibodies are formed.
3. Mother Rh- and Husband Rh-
No risk: If both parents are Rh-negative, the fetus will also be Rh-negative, eliminating the risk of Rh isoimmunization.
First Pregnancy
- Mother Rh-negative, baby Rh-positive: The mother produces IgM antibodies initially, which don’t cross the placenta. After 7 months, IgG antibodies are produced, but the first child is usually safe.
Second Pregnancy
- Rh-negative mother, Rh-positive fetus: The IgG antibodies cross the placenta, causing hemolytic disease of the newborn, which can lead to fetal death.
Prevention of Rh Isoimmunization
Mother Rh-negative, Fetus Rh-positive:
- Give Rh immunoglobulin (RhoGAM) at 28 weeks of pregnancy to prevent the formation of antibodies.
- If the baby is born Rh-positive, administer RhoGAM within 72 hours after delivery to prevent sensitization.
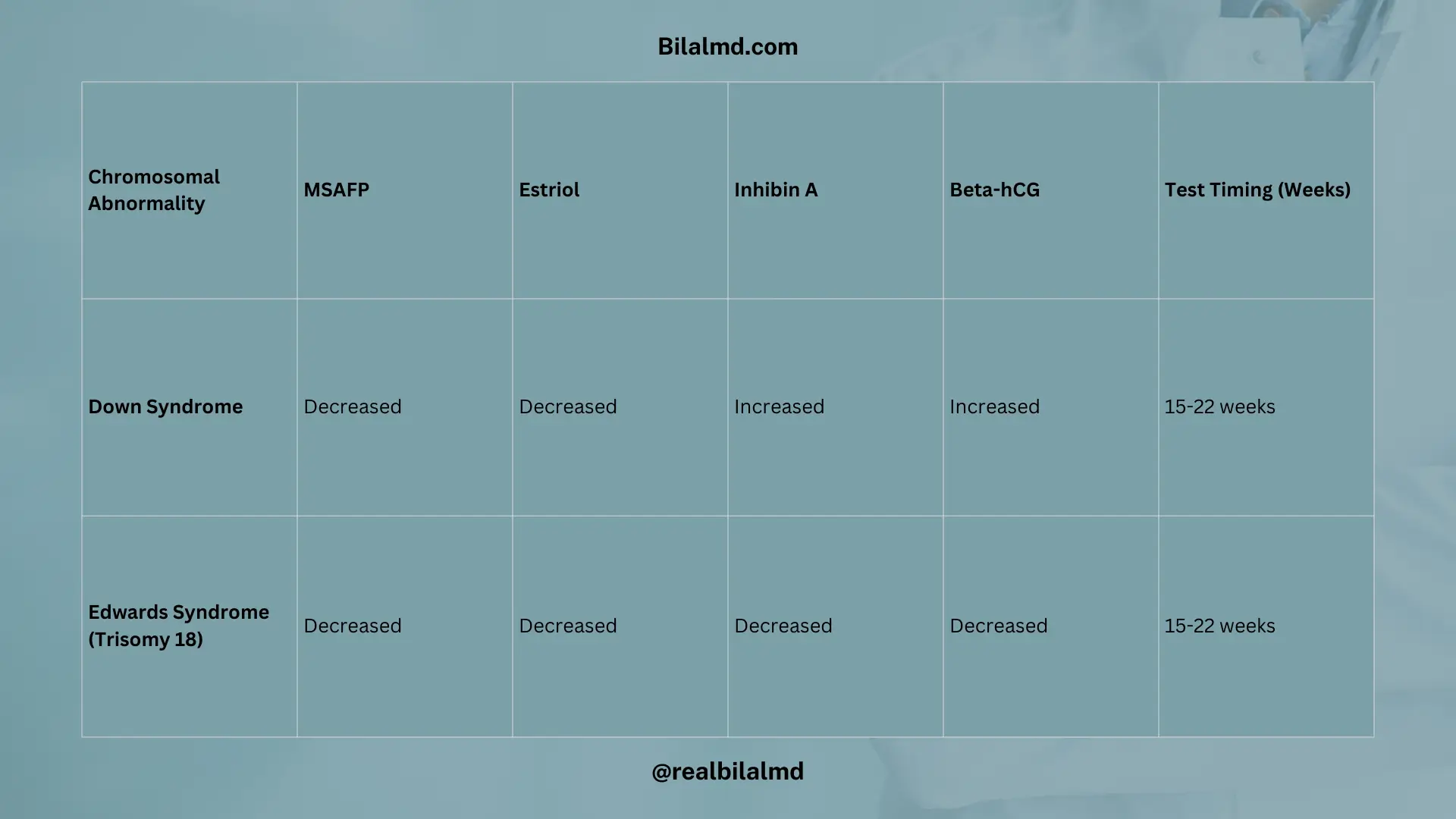
13. Quad Screen Test
Check chromosomal abnormalities between 18 and 22 weeks.
| Chromosomal Abnormality | MSAFP | Estriol | Inhibin A | Beta-hCG | Test Timing (Weeks) |
|---|---|---|---|---|---|
| Down Syndrome | Decreased | Decreased | Increased | Increased | 15-22 weeks |
| Edwards Syndrome (Trisomy 18) | Decreased | Decreased | Decreased | Decreased | 15-22 weeks |
Check your NRE Step 1 result after completing the exam.