Upper Limb Anatomy
The upper limb has three parts:
- Arm (Brachium): This part connects the shoulder to the elbow.
- Forearm (Antebrachium): This part connects the elbow to the wrist. It contains 8 carpal bones.
- Hand (Mannum).
Hand bones in numbers;
- 8 carpels
- 5 metacarpal
- 14 phalanges
1. Nerve Injuries of the Upper Limb
1. Waiter’s tip position (Erb’s Palsy):
Erb’s Palsy is caused by an injury to the upper trunk of the brachial plexus, typically affecting the C5 and C6 nerve roots. It can occur during childbirth (e.g., excessive pulling or traction) or through trauma.
Clinical Features:
- Posture: The arm is held in a characteristic position:
- Medially rotated (internal rotation)
- Adducted (arm close to the body)
- Pronation (forearm rotated so palm faces down)
2. Klumpke’s Palsy (Lower Trunk Injury)
Klumpke’s Palsy is a result of injury to the lower trunk of the brachial plexus, involving the C8 and T1 nerve roots. It’s typically caused by excessive upward pulling or traction on the arm (such as during childbirth or in severe accidents).
Clinical Features:
- Claw hand deformity: Characterized by hyperextension of the metacarpophalangeal joints and flexion of the interphalangeal joints. This occurs due to paralysis of the intrinsic hand muscles, which are mostly innervated by the ulnar nerve.
2. Brachial Plexus Injury and Its Impact on Shoulder Function
- C5, C6, and C7 contribute to the long thoracic nerve and the medial root of the median nerve.
- The long thoracic nerve innervates the serratus anterior, and injury to this nerve results in winging of the scapula.
- Winging of the scapula affects the ability to abduct the arm and can cause deltoid atrophy.
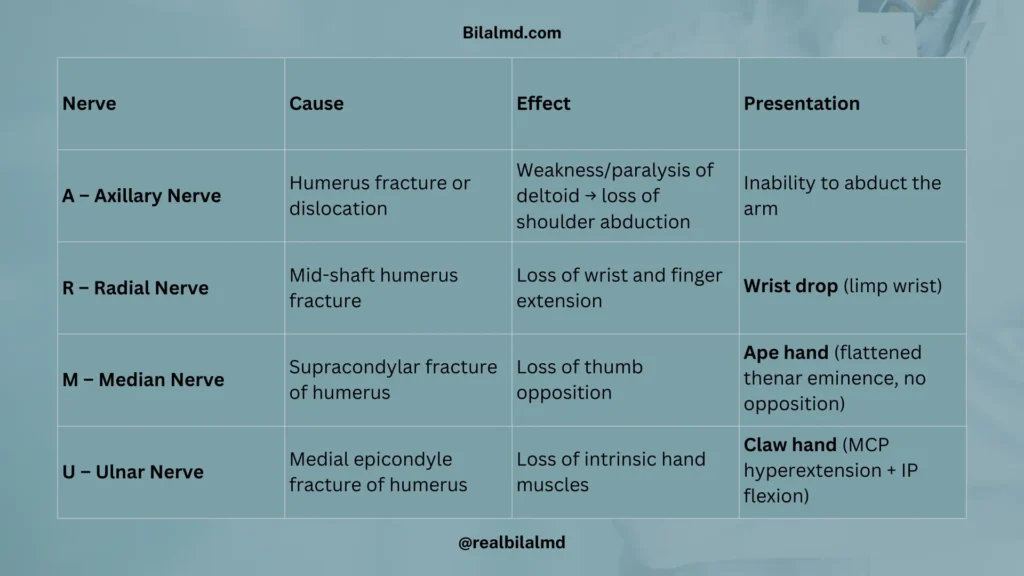
3. ARMU – Nerve Palsy and Their Effects on the Hand and Arm
Remember mnemonic “ARMU“
| Mnemonic | Nerve Palsy | Cause | Effect | Presentation |
|---|---|---|---|---|
| A | Axillary Nerve Palsy | Humerus fracture or dislocation | Weakness or paralysis of the deltoid; loss of shoulder abduction | Inability to raise (abduct) the arm |
| R | Radial Nerve Palsy | Humerus shaft fracture | Wrist drop (inability to extend wrist and fingers) | Wrist hangs limp, no wrist or finger extension |
| M | Median Nerve Palsy | Supracondylar fracture | Ape hand deformity (loss of thumb opposition) | Flattened thenar eminence, inability to oppose thumb |
| U | Ulnar Nerve Palsy | Medial epicondyle fracture | Claw hand deformity (hyperextension of MCP, flexion of IP joints) | Claw hand appearance, loss of intrinsic hand function |
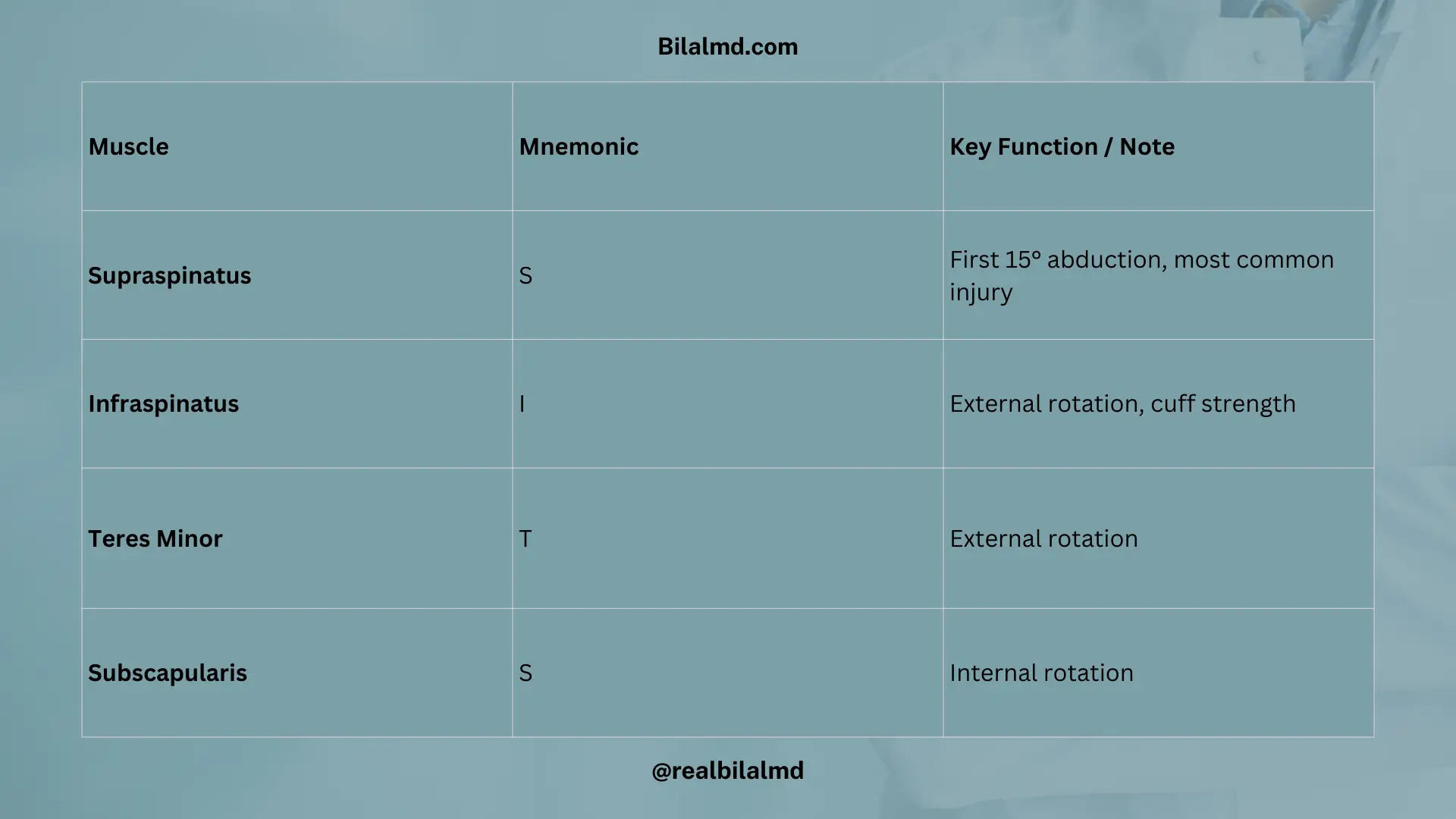
Rotator Cuff Components (Mnemonic: SITS)
| Mnemonic | Muscle | Details |
|---|---|---|
| S | Supraspinatus | Most common injury |
| I | Infraspinatus | |
| T | Teres Minor | |
| S | Subscapularis |
Shoulder Dislocation
- Most common direction: Anterior
- Nerve commonly damaged: Axillary Nerve
4. ARM Muscles and Nerves
Flexors (Muscle mnemonic: BBC)
| Muscle | Innervated by | Blood Supply |
|---|---|---|
| Biceps | Musculocutaneous | Brachial artery |
| Brachialis | Musculocutaneous | Brachial artery |
| Coracobrachialis | Musculocutaneous | Brachial artery |
Extensors
| Muscle | Innervated by |
|---|---|
| Triceps | Radial nerve |
5. Arm Abduction and Associated Muscles and Nerves
| Degree Range | Muscle | Nerve |
|---|---|---|
| 0° to 15° | Supraspinatus | Suprascapular nerve |
| 15° to 90° | Deltoid | Axillary nerve |
| More than 90° | Trapezius | Accessory nerve |

6. Wrist Bones (Carpals)
There are 8 carpal bones in the wrist, arranged in two rows:
1. Proximal Row:
- Scaphoid: Most commonly fractured carpal bone. Can be palpated in the anatomical snuffbox.
- Lunate: Most commonly dislocated. Median nerve injury can occur due to lunate dislocation.
- Triquetral
- Pisiform
2. Distal Row:
- Trapezium
- Trapezoid
- Capitate
- Hamate: Ulnar nerve injury occurs with a fracture of the hamate.

7. Hand Muscles
| 3 1/2 Finger | 1 1/2 Finger |
| Thenar | Hypothenar |
| Opponens Muscle | Interossei (Dorsal Abduction ,Palmar Adduction) |
| Lumbricals (Lateral) | Lumbricals (Medial) |
Veins in the Forearm/Hand
- Basilic Vein: Runs medially and is superficial.
- Cephalic Vein: Runs laterally and drains into the axillary vein.
8. Thigh Region Muscles and Nerves
| Thigh Compartment | Muscles (key ones) | Primary Nerve (+ roots) |
|---|---|---|
| Anterior | Rectus femoris Quadriceps femoris Vastus Lateralis Vastus Medialis Vastus Intermedius | Femoral n. (L2 L3 L4) |
| Medial | Adductor longus Adductor brevis Adductor magnus | Obturator n. (L2 L3 L4) |
| Posterior | Biceps femoris (short head) → Common fibular n. Semimembranosus Semitendinosus | Sciatic n. (L4 L5 S1 S2 S3) |
The sciatic nerve (L4-S3) splits into two branches:
- Tibial Nerve (L4-S3) – continues down the leg.
- Common Fibular (Peroneal) Nerve (L4-S3) – divides at the neck of the fibula into:
- Deep Fibular Nerve
- Superficial Fibular Nerve
| Thigh | Leg |
|---|---|
| Anterior: Femoral Nerve | Anterior: Deep Peritoneal Nerve |
| Medial: Obturator Nerve | Lateral: Superficial Peritoneal Nerve |
| Posterior: Sciatic Nerve (Tibial, Common Peroneal Nerve) | Posterior: Tibial Nerve |
| Common Peroneal Nerve: Divides at the neck of the fibula into Deep Peroneal Nerve and Superficial Peroneal Nerve | Deep Peroneal Nerve: Dorsiflexion (movement upwards) |
| Fracture at Neck of Fibula + Foot Drop: Common Peroneal Nerve Injury | Superficial Peroneal Nerve: Plantar Flexion (movement downwards) |
| Permanent Dorsiflexion Loss: Tibial Nerve Palsy | |
| Posterior Leg: Sciatic Nerve (L4, L5, S1, S2, S3) | Posterior Leg: Tibial Nerve (L4, L5, S1, S2, S3) |
| Vein | Drainage | Usage/Effect |
|---|---|---|
| Great Saphenous Vein | Drains into Femoral Vein | Used for grafting in bypass surgeries |
| Short Saphenous Vein | Drains into Popliteal Vein | Can lead to Deep Vein Thrombosis (DVT) if affected |
9. Abdomen
- Divides at L4: At the level of L4, the abdominal aorta divides into common iliac arteries.
- Continuation of Thoracic Aorta: The abdominal aorta is a continuation of the thoracic aorta.
- Passes through Diaphragm: It passes through the diaphragm at the T12 level.
1. Visceral Branches of the Abdominal Aorta
- From the Front:
- Celiac Trunk
- Superior Mesenteric Artery (SMA)
- Inferior Mesenteric Artery (IMA)
- From the Periphery:
- These branches supply the visceral organs like the intestines, liver, pancreas, and others
2. Fatty Structures
- Mesentery: The mesentery (fatty tissue on the intestine) is supplied by the mesenteric arteries (from the IMA).
- Omentum: The fatty tissue of the omentum is also supplied by the arteries, particularly from the mesenteric arteries.
1. Foregut
The foregut includes the following organs, primarily supplied by the Celiac Trunk:
- Pancreas
- Esophagus
- Stomach
- 2/4 of the Duodenum (first part)
- Liver
- Gallbladder
- Spleen
1. Celiac Trunk (T12)
The Celiac Trunk is a major visceral branch of the abdominal aorta that arises at the T12 level. It supplies the foregut organs.
Branches of the Celiac Trunk:
Supplies the spleen, pancreas, and part of the stomach.
1. Left Gastric Artery:
- Shortest branch of the celiac trunk.
- Clinical Significance: Most commonly affected in gastric ulcers, leading to bleeding.
2. Hepatic Artery:
Divides into:
- Gastroduodenal Artery: Supplies the stomach and duodenum.
- Right Gastric Artery: Supplies the lesser curvature of the stomach.
- Proper Hepatic Artery: Continues towards the liver.
3. Splenic Artery:
- Longest branch of the celiac trunk.
- Supplies the spleen, pancreas, and part of the stomach.
4. Left Gastric Artery (LGA)
- Supplies:
- Lower end of the esophagus.
- Upper half of the lesser curvature of the stomach.
- Clinical Significance:
- Most commonly affected in gastric ulcers, causing bleeding.
5. Hepatic Artery
- Branches:
- Right Gastric Artery: Supplies the lesser curvature of the stomach.
- Gastroduodenal Artery:
- Gives rise to the Superior Pancreaticoduodenal Artery, which supplies the head of the pancreas and duodenum.
- Right Gastroepiploic Artery: Supplies the lower half of the greater curvature of the stomach.
2. Gallbladder
- The gallbladder is attached to the right lobe of the liver.
- Blood Supply: The right hepatic artery supplies the gallbladder.
3. Splenic Artery (Branch of the Celiac Trunk)
- Pancreatic Arteries
- Supplies the pancreas.
- Left Gastroepiploic Artery:
- Supplies the spleen and the upper half of the greater curvature of the stomach.
- Short Gastric Arteries:
- Supplies the fundus of the stomach.
- Gastro-Duodenal Artery
- Clinical Relevance: A common site for duodenal ulcers to cause bleeding due to its proximity to the duodenum.
- Left Gastric Artery (LGA)
- Clinical Relevance: Can cause bleeding in cases of gastric ulcers, particularly due to its supply to the lower esophagus and upper half of the lesser curvature of the stomach.
2. Midgut (Supplied by the Superior Mesenteric Artery (SMA))
- Organs Supplied:
- Duodenum (3rd and 4th parts)
- Jejunum
- Ileum
- Cecum
- Appendix
- Ascending Colon
- Hepatic Flexure
- Transverse Colon (proximal 2/3)
- Retrocecal Colon
1. Superior Mesenteric Artery (SMA) Branches:
- Inferior Pancreaticoduodenal Artery:
- Supplies the head of the pancreas and the 3rd and 4th parts of the duodenum.
- Jejunal Artery:
- Supplies the jejunum.
- Ileocecal Artery:
- Supplies the ileum, cecum, and appendix.
- Right Colic Artery:
- Supplies the ascending colon, hepatic flexure, and the proximal 2/3 of the transverse colon.
- Middle Colic Artery
- Function: Supplies blood to the hepatic flexure and the proximal 2/3 of the transverse colon.
2. Clinical Correlation
- Abdominal Angina: Caused by SMA occlusion, leading to insufficient blood supply to the intestines, especially during digestion.
- Head of Pancreas: Receives blood supply from both the Celiac Trunk and the Superior Mesenteric Artery (SMA).
3. Hindgut Vascular Supply
| Region | Artery | Blood Supply | Clinical Relevance |
|---|---|---|---|
| Transverse Colon | Inferior Mesenteric Artery (IMA) | Supplies blood to the transverse colon (L3) | |
| Splenic Flexure | Left Colic Artery | Supplies distal 1/3 of the transverse colon and splenic flexure | Known as the watershed area, vulnerable to ischemia |
| Descending Colon | Left Colic Artery | Supplies the descending colon from the splenic flexure to the sigmoid colon | |
| Sigmoid Colon | Sigmoid Arteries | Supplies the sigmoid colon | |
| Rectum | Superior Rectal Artery | Supplies the upper part of the rectum |
1. Paired branches of abdominal aorta
| Vessel | Branch/Function | Clinical Relevance |
|---|---|---|
| Renal Arteries | Branch at L1-L2, entering the renal hilum | Right renal artery is slightly longer than the left renal artery |
| Suprarenal Arteries | Supply blood to the adrenal glands | Supplied by branches from the phrenic artery and renal arteries |
| Gonadal Artery | Female: Supplies the ovaries Male: Supplies the testes | Left Testicular vein drain to the left renal vein, Varicocele can occur when SMA aneurysm compresses the left renal vein |
| Region | Artery | Vein | Blood Supply/Drainage |
|---|---|---|---|
| Foregut | Celiac Trunk | Portal Vein | Supplies blood to the foregut (includes esophagus, stomach, liver, pancreas) |
| Midgut | Superior Mesenteric Artery (SMA) | Superior Mesenteric Vein (SMV) | Supplies blood to the midgut (includes duodenum, jejunum, ileum) |
| Hindgut | Inferior Mesenteric Artery (IMA) | Inferior Mesenteric Vein (IMV) | Supplies blood to the hindgut (includes descending colon, sigmoid colon, rectum) |
2. Portal vein
| Portal Vein | Details |
|---|---|
| Formation | Formed by the union of the Superior Mesenteric Vein (SMV) and Splenic Vein (SV), with the Inferior Mesenteric Vein (IMV) contributing as well. |
| Location | Behind the neck of the pancreas. |
| Valves | The portal vein has no valves. |
| Portosystemic Anastomosis | Anastomosis between the portal system veins and systemic veins. |
| Obstruction in Portal Vein | In cases of portal hypertension or obstruction, blood bypasses to other veins through portosystemic anastomoses (e.g., esophageal varices). |
3.Portosystemic Shunting and Its Clinical Signs
| Site | Portal Side (Vein) | Caval Side (Vein) | Clinical Sign |
|---|---|---|---|
| Lower End of Esophagus | Left Gastric Vein | Azygos Vein | Esophageal Varices |
| Upper Part of Rectum | Inferior Mesenteric Vein | Inferior Rectal Vein (IRV) | Internal Hemorrhoids |
| Umbilicus | Paraumbilical Vein | Anterior Abdominal Vein | Caput Medusa |
4. IVC and Venous Drainage
- Superior Vena Cava (SVC)
- Bifurcates at L5.
- Inferior Vena Cava (IVC):
- Formed by the union of the common iliac veins at L5.
- Ascends along the midline and passes through the diaphragm at the T8 level.
- Receives blood indirectly from the following regions:
- Lower Limb
- Pelvis
- Abdomen
- Perineum
5. Gonadal Veins:
- Right Gonadal Vein: Drains directly into the IVC.
- Left Gonadal Vein: Drains into the splenic vein, which then drains into the IVC.
Here are other materials for NLE NRE step 1
4. Perinium
- The perineum is a diaphragm-shaped space between the anus and reproductive organs.
- Best studied in the lithotomy position.
1. Pelvic Diaphragm (Levator Ani)
- Function:
- The pelvic diaphragm (mainly the levator ani muscles) provides support to the pelvic organs.
- The pudendal nerve (S2, S3, S4) and the internal pudendal artery supply the pelvic region, providing anesthesia for procedures such as episiotomies.
- Cutting is performed medial to lateral for some procedures.
2. Muscles of the Pelvic Diaphragm:
- Puborectalis Muscle:
- Weakness in this muscle can lead to fecal incontinence.
- Pubococcygeus Muscle:
- Weakness in this muscle can contribute to urinary incontinence.
- Iliococcygeus Muscle:
- Less involved in supporting the pelvic floor compared to others.
- Ischiococcygeus Muscle:
- Plays a smaller role in supporting the pelvic floor.
1. Urogenital Triangle (UG Triangle)
The Urogenital Triangle (UG Triangle) is located above the imaginary line drawn from the anterior aspect of the perineum.
Fascia of the Perineum
- Fascia Scarpa (from the abdomen):
- Extends to the scrotum, where it is called Dartos Fascia.
- Further extension into the perineum is known as Colle’s Fascia, which then meets the perineal membrane, forming the superficial pouch.
- Clinical Relevance:
- If there is damage to the penile urethra, urine leakage can occur into the scrotum, axilla, or thigh due to the continuity of Colle’s Fascia.
2. Boundaries of the Urogenital Pouch:
- Roof:
- Superior layer of the UG pouch.
- Floor:
- Perineal membrane (inferior boundary of the UG pouch).
- Anterior Boundary:
- Transverse perineal ligament.
- Posterior Boundary:
- Fusion of the superior and inferior layers of the pouch.
3. Contents of the Deep Pouch:
- Membranous Urethra:
- Part of the urethra located within the deep pouch.
- External Urethral Sphincter Muscle:
- Surrounds the membranous urethra, responsible for controlling urine flow.
- Bulbourethral Glands (Cowper’s Glands):
- These glands secrete a fluid that lubricates the urethra during ejaculation.
- Deep Transverse Perineal Muscle:
- Provides support to the pelvic floor and is involved in maintaining the integrity of the UG pouch.
2. Superficial Perineal Pouch
The superficial perineal pouch is the space below the deep perineal pouch.
1. Boundaries of the Superficial Perineal Pouch:
- Roof:
- Perineal membrane.
- Floor:
- Colle’s fascia (forms the floor of the pouch).
- Anterior Wall:
- Deficient (no specific structure to form the anterior boundary).
- Posterior Wall:
- Formed by the fusion of Colle’s fascia and the perineal membrane.
2. Contents of the Superficial Perineal Pouch:
- Penile Urethra:
- Extends through the upper part of the thigh, anterior abdominal wall, scrotum, and superficial perineal pouch.
- Muscles:
- Bulbospongiosus: Surrounds the bulb of the penis and contributes to erection.
- Ischiocavernosus: Covers the crus of the penis, helps with erection.
- Bartholin’s Gland (in females):
- Secretes mucus to lubricate the vaginal opening.
- Erectile Tissue:
- Penis in males.
- Clitoris in females.
- Bulb of the Penis:
- Located within the superficial perineal pouch, part of the erectile tissue in males.
| Mnemonic | Urethral Injury | Location/Specifics |
|---|---|---|
| MUD | Membranous Urethral Injury | Deep injury, typically more proximal. |
| PUS | Penile Urethral Injury | Specific to the penile urethra, often due to trauma or fractures. |
3. Anal triangle
| Feature | Details |
|---|---|
| Location | Lies below the imaginary line between the ischial tuberosities. |
| Scrotal Tuberous Ligament | Present in the region, providing support to the scrotum. |
| Contents | – Opening of the anus |
| – External anal sphincter muscle | |
| – Ischiorectal fossa containing fat and connective tissue. |
5. Neuroanatomy
- Brain
- Spinal Cord
- Brainstem
- Medulla Oblongata
- Midbrain
- Pons
| Region | Part | Details |
|---|---|---|
| Forebrain | Telencephalon | |
| Diencephalon | ||
| Midbrain | Mesencephalon | |
| Hindbrain | Metencephalon | Includes the pons and cerebellum, responsible for motor control, coordination, and balance. |
| Myelencephalon | Contains the medulla oblongata, responsible for vital functions like breathing, heart rate, and blood pressure. |
1. CSF
| Feature | Details |
|---|---|
| Characteristics | Colorless, odorless fluid |
| Functions | – Provides protection to the brain |
| – Prevents injury to the brain | |
| – Provides nutrition to the brain | |
| – Removes waste from the brain | |
| – Helps in certain diagnosis (e.g., through lumbar puncture) | |
| CSF Synthesis | Synthesized by ependymal cells present in the 4 ventricles |
| Max CSF Location | Subarachnoid space contains the maximum amount of CSF |
2. CSF Circulation
| Region | CSF Flow and Blockage | Details |
|---|---|---|
| Forebrain | CSF in the lateral ventricle flows to the 3rd ventricle via Foramen of Monro. | Foramen of Monro accounts for 10% of blockage. |
| Midbrain | From the 3rd ventricle, CSF flows to the 4th ventricle through the Cerebral Aqueduct. | Cerebral aqueduct accounts for 90% blockage in the midbrain. |
| Hindbrain | In the hindbrain, there are Foramen Magendie and Foramen Luschka for CSF to enter the subarachnoid space. | These allow CSF flow into the subarachnoid space. |
| CSF Absorption | CSF is absorbed by subarachnoid granulations and then enters the venous system. | These granulations help to drain CSF into the venous system. |
| Condition | Details |
|---|---|
| Communicating Hydrocephalus | There is no obstruction in any of the foramen (e.g., Foramen of Monro, Cerebral Aqueduct, Foramen Magendie, Foramen Luschka). |
| The problem arises from decreased absorption of cerebrospinal fluid (CSF) by the subarachnoid granulations. | |
| This results in an accumulation of CSF in the ventricles. |
3. Cranial Nerves and Their Clinical Significance
1. Olfactory Nerve (CN I)
- Type: Sensory
- Function: Responsible for the sense of smell. The olfactory bulb processes the smell sensation.
- Clinical Significance:
- Anosmia: Loss of smell sensation.
2. Optic Nerve (CN II)
- Type: Sensory
- Function: Responsible for vision and light reflex (CN 3).
- The optic nerve receives signals and constricts the pupil via CN 3 (afferent to efferent).
- Clinical Significance:
- Loss of vision.
- Loss of light reflex: Can be damaged in Multiple Sclerosis (MS).
3. Oculomotor Nerve (CN III)
- Type: Motor
- Function:
- Controls levator palpebrae superioris (opening eyelid).
- Controls superior rectus, inferior rectus, medial rectus, and inferior oblique muscles (eye movement).
- Controls sphincter pupillae (pupil constriction) and ciliary muscle (accommodation).
- Clinical Significance:
- Ptosis: Drooping eyelid.
- Divergent squint: Misalignment of the eyes.
- Dilation of pupil: Can indicate damage to CN III.
4. Trochlear Nerve (CN IV)
- Type: Motor
- Function:
- Controls the superior oblique muscle (responsible for downward and lateral eye movement).
- Works in coordination with superior rectus (SR), inferior rectus (IR), and medial rectus (MR) muscles for proper eye movement and alignment.
- Clinical Significance:
- Convergent squint: Eyes point inward (due to imbalance in muscle control).
- Divergent squint: Eyes point outward.
5. Trigeminal Nerve (CN V)
- Type: Mixed (Sensory + Motor)
- Divisions:
- Ophthalmic Division (V1): Sensory – Provides sensation to the forehead, scalp, and eyelids.
- Maxillary Division (V2): Sensory – Provides sensation to the maxillary area, including the nose, upper teeth, gums, and lips.
- Mandibular Division (V3): Sensory + Motor – Provides sensation to the lower lip, lower teeth, gums, and mandible. Also controls muscles of mastication (chewing).
- Origin: Arises from the pons in the brainstem.
Trigeminal Nerve (CN V) – Functions
| Function | Details |
|---|---|
| 1. Corneal Reflex | Along with CN VII (facial nerve), the trigeminal nerve helps initiate the blink reflex when the cornea is touched. |
| 2. General Sensation (Maxillary Area) | Provides sensation of the maxillary region (nose, upper teeth, gums, and lips) via V2. |
| 3. Sensation of Lower Lip, Teeth, and Mandible | Provides sensation to the lower lip, lower teeth, gums, and mandible via V3. |
| 4. Sensation from Scalp to Eyelid | Controls sensation like touch and temperature from the scalp to the eyelid. |
Motor innervation
| Muscle | Function |
|---|---|
| Temporalis | Elevates the mandible (helps close the mouth) |
| Masseter | Elevates the mandible (helps close the mouth) |
| Medial Pterygoid | Elevates the mandible (helps close the mouth) |
| Lateral Pterygoid | Depresses the mandible (helps open the mouth) |
| Muscle | Function/Details | Innervation |
|---|---|---|
| Digastric Muscle | A two-bellied muscle in the neck that helps with depression of the mandible (opening the mouth) and assists with swallowing. | Anterior Belly: Innervated by CN V. Posterior Belly: Innervated by CN VII. |
7. Facial Nerve (CN VII)
Origin:
- Arises from the pons-medulla junction.
Functions:
- Facial Expression:
- Controls all facial expressions.
- Blink Reflex:
- Works with CN VI (Abducens) to control the blink reflex.
- Posterior Belly of Digastric Muscle:
- Innervates the posterior belly of the digastric muscle, contributing to jaw movements.
- Stapedius Muscle:
- Innervates the stapedius muscle, which helps in controlling sound intensity.
- Dysfunction can result in hypersensitivity to sound, where even normal sounds feel extremely loud.
Tongue Sensation:
1. Anterior 2/3 of the Tongue:
- Taste Sensation: Mediated by CN VII (Facial Nerve) via the chorda tympani.
- General Sensation: Mediated by CN V (Trigeminal Nerve) via the lingual nerve.
2 .Posterior 1/3 of the Tongue:
- Innervation:
- Both general and special sensation are mediated by the Glossopharyngeal Nerve (CN IX).
- Parasympathetic Innervation:
- Lacrimal Glands: Responsible for tear production.
- Sublingual and Submandibular Glands: Responsible for saliva production.
- Additional Functions:
- Orbicularis Oculi Muscle:
- Involved in the closing of the eyes, mediated by CN VII (Facial Nerve).
- Orbicularis Oculi Muscle:
Clinical Significance:
- Loss of Forehead Wrinkles: Due to weakened frontalis muscle.
- Inability to Close Eye: Due to paralysis of orbicularis oculi.
- Loss of Facial Expression: Overall facial paralysis affecting muscles of expression.
- Asymmetry of Mouth: Drooping or inability to smile symmetrically.
- Change in Taste Sensation: Loss of taste sensation on the anterior 2/3 of the tongue.
8. Vestibulocochlear Nerve (Cranial Nerve VIII)
- Nature: Sensory
- Function:
- Balance: Maintains equilibrium through the vestibular system.
- Hearing: Transmits sound information via the cochlear system.
Clinical Significance:
- Outer & Middle Ear Issues:
- Can lead to conductive hearing loss due to problems in the external or middle ear.
- Inner Ear Issues:
- Results in sensorineural hearing loss (damage to the cochlea or auditory nerve).
- May cause tinnitus (ringing in the ears) and vertigo (a sense of spinning or dizziness).
- Nystagmus:
- A condition where there is involuntary eye movement (often described as “dancing eyes“), typically due to vestibular dysfunction.
- Tumors:
- Acoustic Neuroma (also called vestibular schwannoma or neurolimoma) is a benign tumor of CN 8, causing hearing loss, tinnitus, and balance issues.
9. Glossopharyngeal Nerve (Cranial Nerve IX)
- Nature: Mixed (Sensory + Motor) with Parasympathetic fibers.
Function:
- Salivary Gland (Parotid Gland):
- Stimulates the parotid gland via the lesser petrosal nerve for saliva production.
- Pharyngeal Muscles:
- Stylopharyngeus muscle is innervated by CN 9; all other pharyngeal muscles are controlled by the vagus nerve (CN X).
- Sensory Function:
- General and Special Sensation: Responsible for the sensation of the posterior 1/3 of the tongue (both taste and general sensation).
- Regulation of Blood Pressure:
- Plays a role in controlling short-term blood pressure through its afferent fibers to the carotid sinus (baroreceptor function).
Clinical Significance:
- Damage:
- Loss of Gag Reflex: A lesion to CN IX, along with CN X (vagus nerve), can result in the loss of the gag reflex.
- Uvula Deviation: The uvula will deviate toward the unaffected side in cases of CN IX damage.
10 .Vagus Nerve (Cranial Nerve X)
- Nature: Mixed (Sensory + Motor)
- Origin: Medulla Oblongata
Function:
- Pharyngeal Muscles:
- Innervates all pharyngeal muscles except the stylopharyngeus (which is innervated by the glossopharyngeal nerve, CN IX).
- Tongue Muscle:
- Innervates the palatoglossus muscle of the tongue.
- Laryngeal Muscles:
- All laryngeal muscles are innervated by the recurrent laryngeal nerve (RLN), except for the cricothyroid muscle, which is innervated by the external laryngeal nerve.
- Regulation of Short-Term Blood Pressure:
- Plays a role in controlling short-term blood pressure through afferent fibers from the carotid body.
- Stomach:
- Innervates parietal cells in the stomach, releasing acetylcholine (ACh) to stimulate HCl secretion.
- Cushing Ulcer:
- Associated with increased intracranial pressure (ICP) leading to vagus nerve damage, resulting in gastric ulcers (Cushing ulcers).
Clinical Significance:
- Dysphagia: Difficulty swallowing due to impaired motor function in the pharynx and larynx.
- Hoarseness of Voice:
- Caused by damage to the recurrent laryngeal nerve (RLN), affecting the vocal cords.
- Loss of Gag Reflex:
- Occurs in conjunction with damage to the glossopharyngeal nerve (CN IX).
- Uvula Deviation:
- In cases of vagus nerve injury, the uvula deviates toward the unaffected side.
11. Accessory Nerve (Cranial Nerve XI)
- Nature: Motor
- Origin:
- Cranial Part: Arises from the medulla (does not merge with the vagus nerve).
- Spinal Part: Originates from the spinal cord and passes through the foramen magnum.
Function:
- Accessory Spinal Part:
- Sternocleidomastoid Muscle: Facilitates head rotation.
- Trapezius Muscle:
- Assist in shoulder elevation.
- Damage to the accessory nerve can result in a dropped shoulder, making tasks like combing hair difficult.
12. Hypoglossal Nerve (Cranial Nerve XII)
- Nature: Motor
- Function:
- Innervates all muscles of the tongue, except the palatoglossus.
- Pathway:
- Cerebellum: 1st and 2nd order neurons to the cerebellum.
- Brainstem: The 3rd to 12th cranial nerves are associated with the brainstem.
- Posterior Origins: 4th and above nerves originate from the posterior part.