Our bodies have a special system called the “endocrine system“. It’s like a messenger service that uses special chemicals called hormones.
1. Pituitary gland
Pituitary gland has 2 lobe;
- Anterior (front) lobe
- Posterior (back) lobe
1. Anterior (front) lobe by surface ectoderm
Anterior lobe makes hormones like
- Growth hormone for growth
- TSH our body uses energy
- Prolactin for milk production
- Acth
- GnH
2. Posterior (back) lobe by Neuroectoderm
Posterior lobe stores hormones by Hypothalamus.
- ADH (vasopressin)
- Oxytocin
2. Natural Contraceptive Hormone
1. Prolactin
Symptoms of high prolactin (Hyperprolactinemia):
- Loss of libido
- Galactorrhea (abnormal milk production)
- Amenorrhea (absence of menstruation)
2. Prolactinoma:
Benign pituitary tumor that secretes excessive prolactin.
Treatment for Prolactinoma:
Dopamine agonists like:
- Cabergoline
- Bromocriptine

3. Growth Hormone (GH) Disorders:
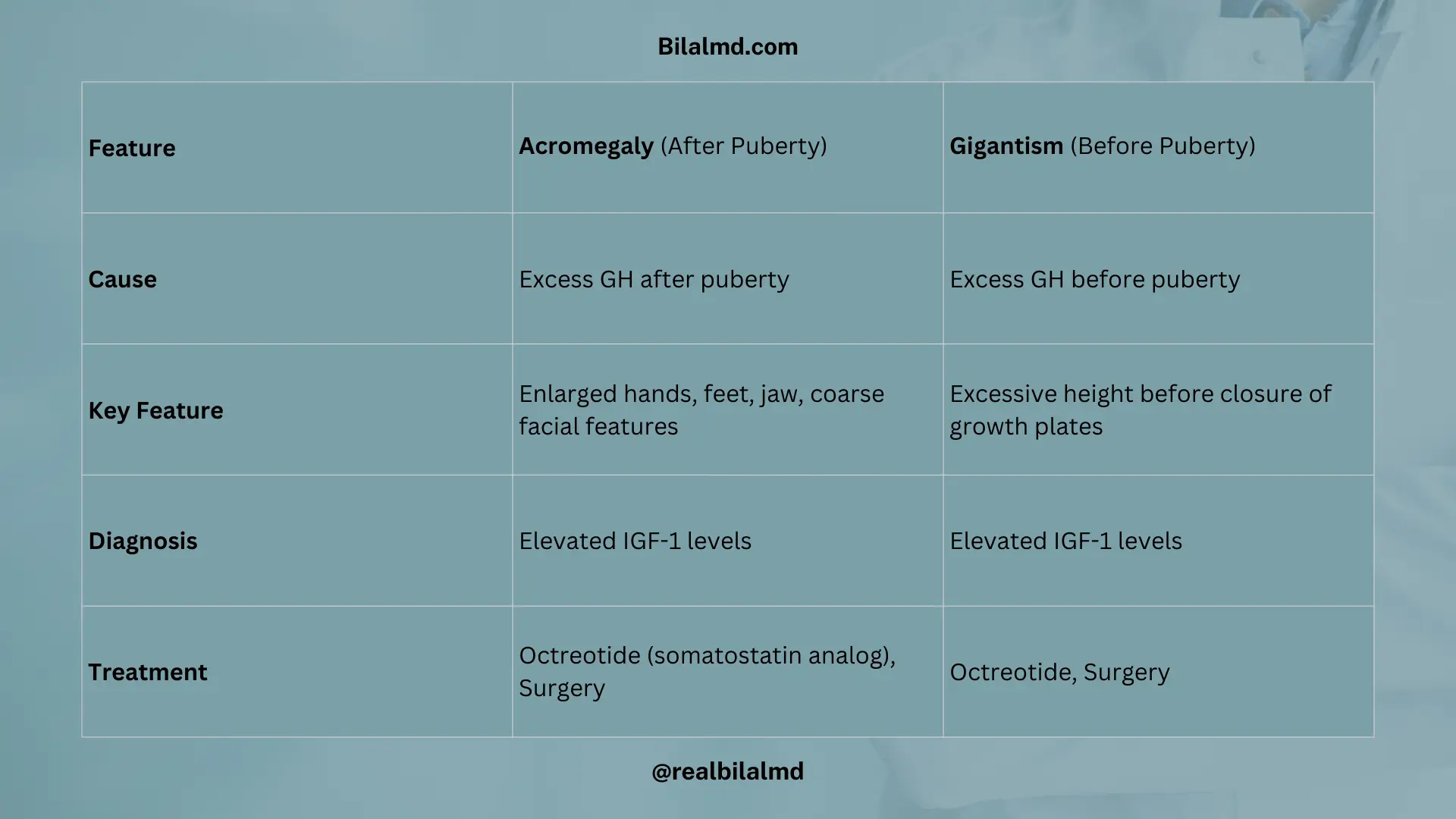
- Acromegaly (GH increases after puberty):
- Cause: Excess GH after puberty leads to acromegaly.
- Diagnosis: IGF-1 levels are elevated.
- Treatment:
- Octreotide (somatostatin analog)
- Surgery
- Gigantism (GH increases before puberty):
- Cause: Excess GH before puberty leads to gigantism (excessive growth in height before the closure of growth plates).
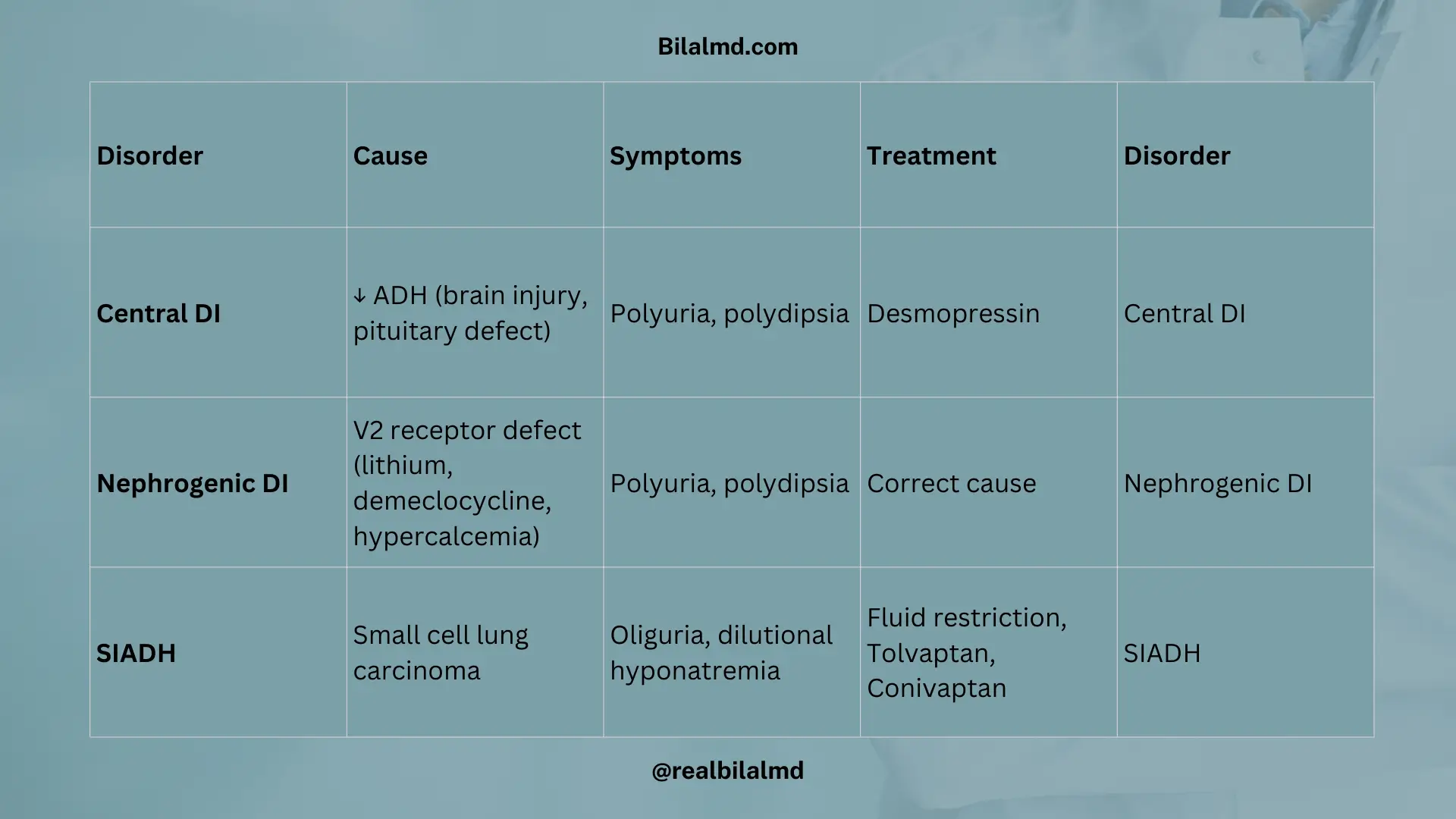
4. Diabetes Insipidus (DI)
1. Central Diabetes Insipidus (CDI)
Cause
Often caused by brain injury or a defect in the hypothalamus or pituitary gland, leading to a lack of ADH (Antidiuretic Hormone) production or release.
Symptoms
- Polyuria (excessive urination)
- Polydipsia (excessive thirst)
Treatment
Desmopressin acetate (an ADH analogue) helps replace the missing ADH
2. Nephrogenic Diabetes Insipidus (NDI)
Cause
Due to a genetic mutation or damage to the kidney’s V2 receptors
Factors contributing to NDI
- Demeclocycline: Damages the V2 receptor.
- Lithium toxicity: Commonly associated with prolonged use of lithium for bipolar disorder.
- Hypercalcemia: High calcium levels can impair kidney function, contributing to NDI.
3. SIADH (Syndrome of Inappropriate Antidiuretic Hormone)
Cause
Often associated with small cell lung carcinoma (SCLC), especially in patients with a history of chronic smoking, weight loss, and hemoptysis (coughing up blood).
Symptoms
- Lack of urine production (oliguria).
- Dilutional hyponatremia (low sodium levels in the blood due to excess water retention).
Treatment
- Resistant to water intake (limit water consumption).
- Tolvaptan and Conivaptan: These are vasopressin receptor antagonists that help reduce the effects of ADH and treat the condition.
- Oxytocin: Used for milk ejection and uterine contractions, also useful in preventing postpartum hemorrhage (PPH).
5. Oxytocin:
Helps in:
- Milk ejection during breastfeeding.
- Uterine contractions, especially during labor.
- Prevention of postpartum hemorrhage (PPH).
6. Thyroid Gland (Ectoderm)
- Follicular Cells: Produce T3 (triiodothyronine) and T4 (thyroxine), which regulate metabolism. Levothyroxine is a synthetic T4 used for hypothyroidism.
- Parafollicular (C) Cells: Produce calcitonin, which lowers blood calcium levels.
| T3 | T4 |
| 3 iodine | 4 iodine |
| Biological active | Less active |
| 7% in serum | 93% in serum |
| Can’t convert to T4 | Convert to T3 |
| Short half life | Long half life |
Hypothalamus Pituitary Thyroid Axis
- Hypothalamus makes TRH
- Ant. pituitary makes TSH
- Thyroid makes T3, T4
Thyroid problem = Primary problem
- Primary hyperthyroidism in which thyroid makes too much T3 and T4
- Primary hypothyroidism in which thyroid doesn’t make enough T3 and T4
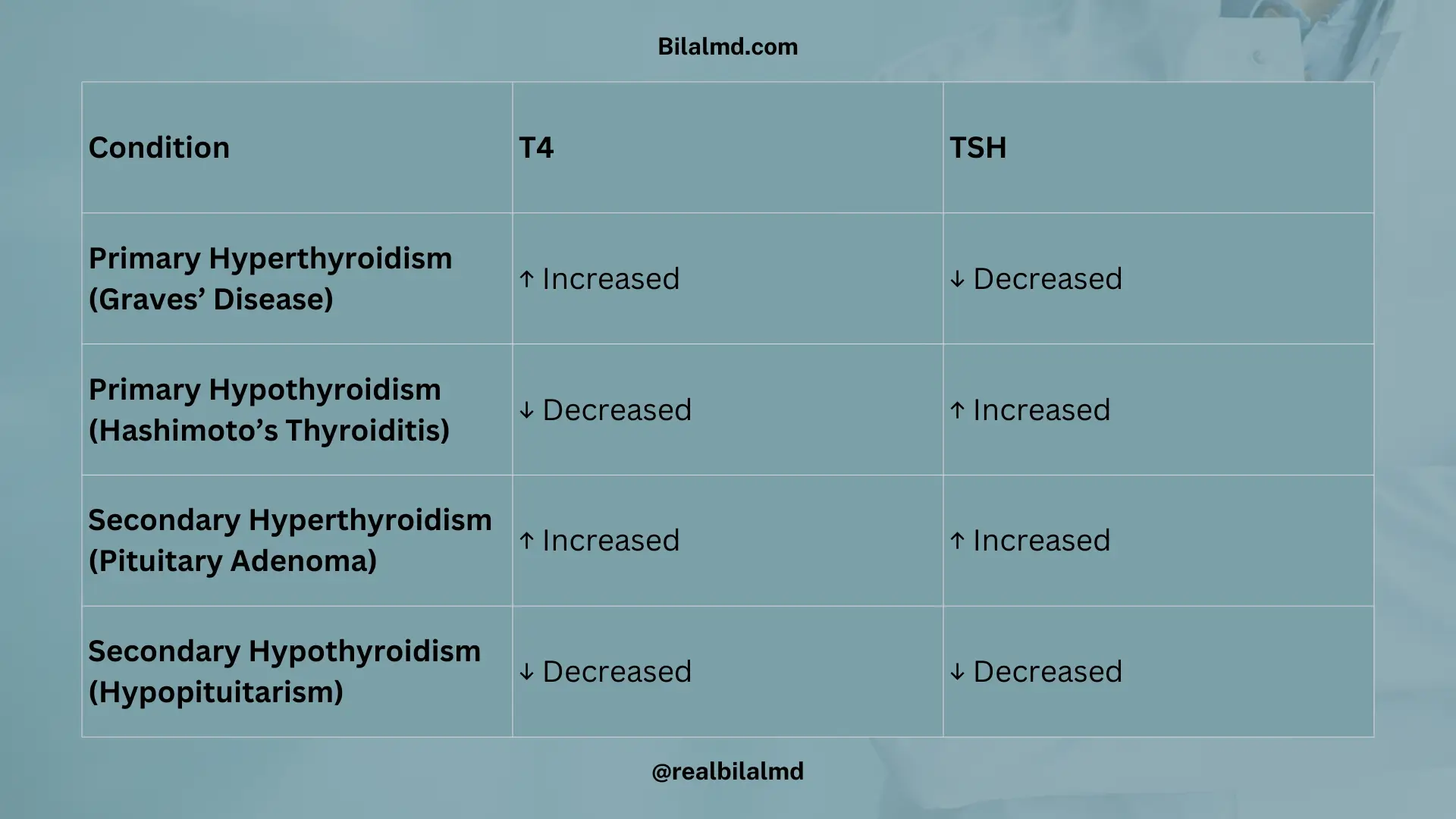
| T4 | TSH | Condition |
|---|---|---|
| Increase | Decrease | Primary Hyperthyroidism (Graves’ Disease) |
| Decrease | Increase | Primary Hypothyroidism (Hashimoto’s Thyroiditis) |
| Increase | Increase | Secondary Hyperthyroidism (Pituitary Adenoma) |
| Decrease | Decrease | Secondary Hypothyroidism (Hypopituitarism) |
Treatment:
- Prophylthiouracil (PTU):
- Action: Inhibits TPO (thyroid peroxidase) and prevents conversion of T4 to T3.
- Use: Preferred during 1st trimester of pregnancy due to safety concerns with other drugs.
- Carbimazole / Methimazole:
- Action: Inhibits thyroid hormone production by blocking TPO.
- Use: Preferred for 2nd and 3rd trimesters of pregnancy.
- Propranolol:
- Action: Reduces palpitations and decreases T4 to T3 conversion.
- Note: Not recommended in asthma as it may worsen respiratory symptoms.
Thyroid Conditions:
- Subacute Thyroiditis (De Quervain’s Thyroiditis):
- Symptoms: Painful thyroid, fever, sore throat, and cough.
- Treatment: NSAIDs to reduce pain and inflammation.
- Thyroid Storm:
- Symptoms: Hyperthyroidism with stress and aggressive symptoms.
- Treatment: Requires immediate medical attention, including antithyroid medications, beta-blockers (like propranolol), and supportive care.
Here are other materials for NLE NRE step 1
7. Parathyroid Gland
- Number and Location:
- 4 parathyroid glands behind the thyroid:
- 2 superior glands (from the 4th pharyngeal pouch) – congenital issues with formation are rare.
- 2 inferior glands (from the 3rd pharyngeal pouch) – can be affected in DiGeorge Syndrome.
- 4 parathyroid glands behind the thyroid:
- Parenchymal Cells (Chief Cells):
- These cells release parathyroid hormone (PTH).
Calcium Regulation:
- Calcium (Ca²⁺) decreases → signals the release of PTH to stabilize calcium levels.
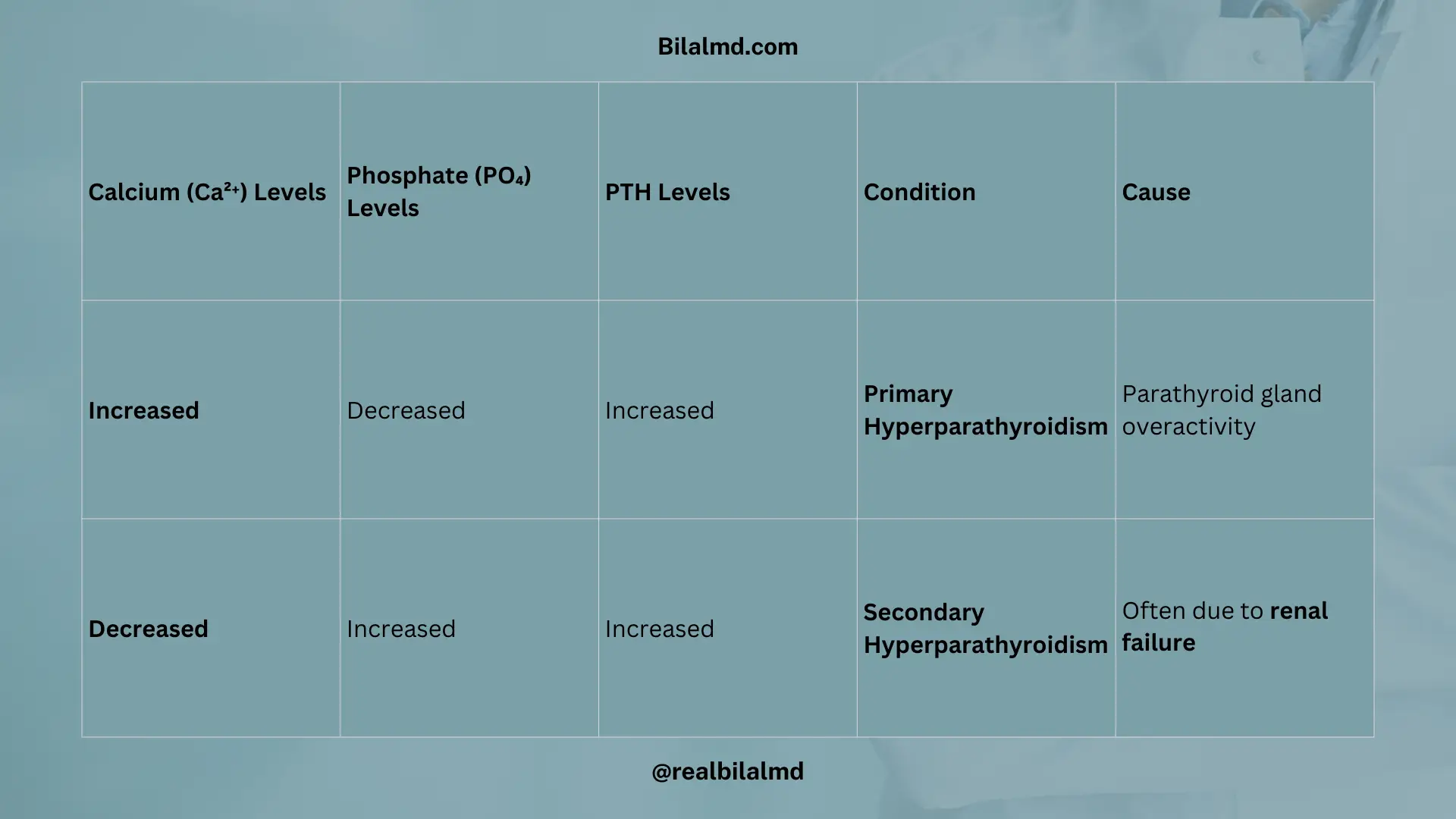
| Calcium (Ca²⁺) Levels | Phosphate (PO₄) Levels | PTH Levels | Condition | Cause |
|---|---|---|---|---|
| Increased | Decreased | Increased | Primary Hyperparathyroidism | Parathyroid gland overactivity |
| Decreased | Increased | Increased | Secondary Hyperparathyroidism | Often due to renal failure |
8. Diabetes
1. Hyperglycemia + Insulin Resistance:
- 3 P’s of Diabetes (commonly seen in both DM1 and DM2):
- Polyuria (frequent urination)
- Polydipsia (excessive thirst)
- Polyphagia (increased hunger)
- Additional Symptoms:
- Weight loss (despite increased appetite, common in Type 1 Diabetes)
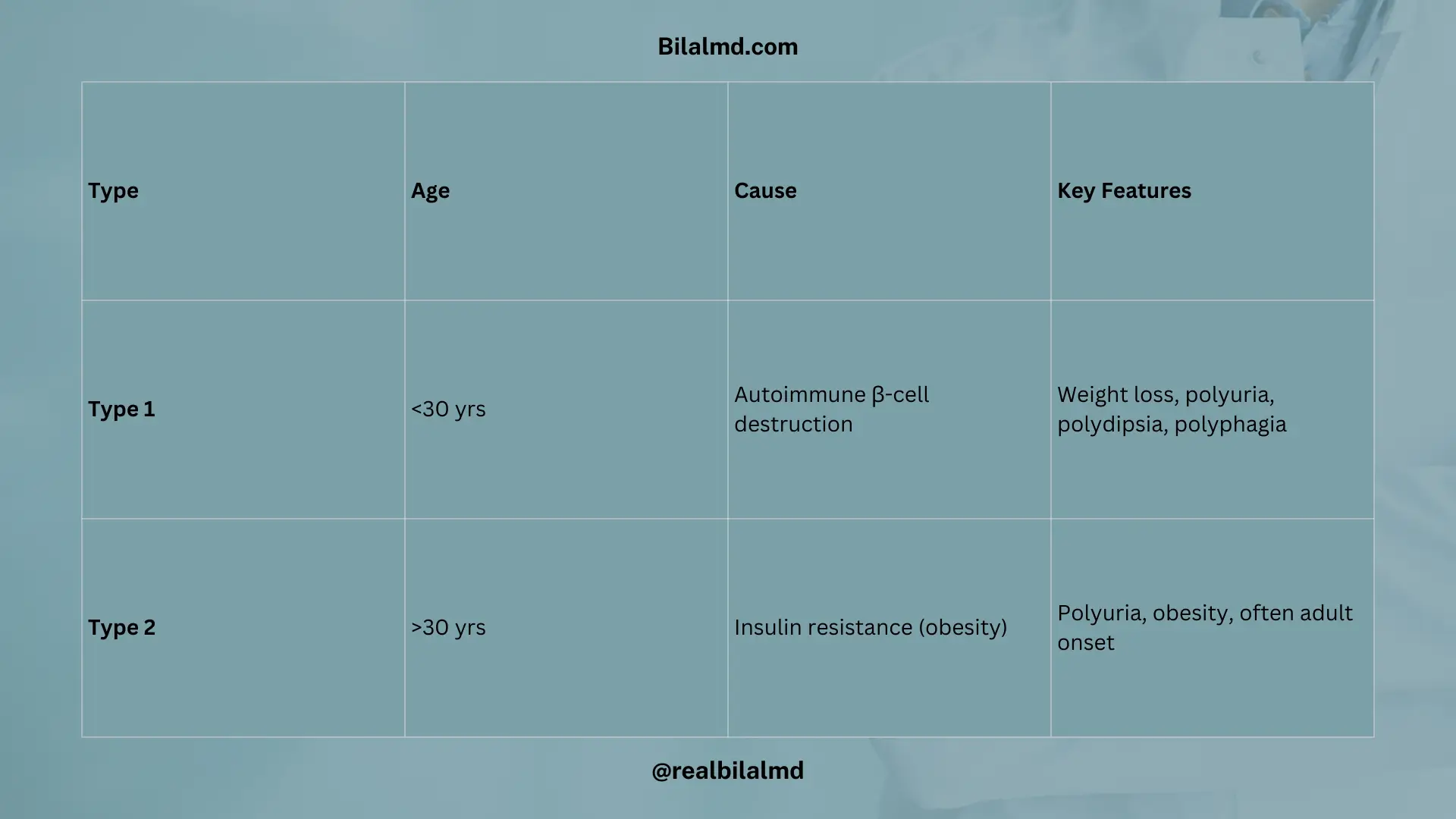
Type 1 Diabetes (DM1):
- Age: Typically <30 years (often diagnosed in childhood or adolescence).
- Cause: Genetic predisposition, often with autoimmune destruction of pancreatic beta cells leading to absolute insulin deficiency.
- Known as Juvenile Diabetes.
Type 2 Diabetes (DM2):
- Age: Typically >30 years (more common in adults).
- Cause: Insulin resistance often due to obesity (fatty tissue disrupts insulin signaling).
- Often associated with lifestyle factors.
2. Classification of insulin
- Ultra-Short Acting Insulin: Aspart, Lispro
- Short-Acting Insulin: Humulin R
- Intermediate-Acting Insulin: NPH (Neutral Protamine Hagedorn)
- Long-Acting Insulin: Glargine
Metformin for Type 2 Diabetes (DM2):
- Medications: Metformin (a biguanide) is commonly prescribed for DM2, especially in obese patients.
- Mechanism: It reduces hepatic glucose production and increases insulin sensitivity.
- Contraindications:
- Lactic acidosis (a rare but serious complication).
- Renal failure (impaired kidney function increases the risk of lactic acidosis).
3. Oral Hypoglycemic Agents:
- SGLT2 Inhibitors (Act on the Kidney):
- Mechanism: They block the Sodium-Glucose Co-Transporter 2 (SGLT2) in the proximal convoluted tubule (PCT) of the kidney, reducing glucose reabsorption and increasing glucose excretion in the urine.
- Examples:
- Empagliflozin
- Dapagliflozin
- Sulfonylureas (Act on Beta Cells):
- Mechanism: They stimulate the beta cells of the pancreas to release insulin, regardless of blood glucose levels.
- Examples:
- Glyburide
- Glimepiride
- Tolbutamide
- Thiazolidinediones (Glitazones):
- Examples: Pioglitazone, Rosiglitazone
- Mechanism: Improves insulin sensitivity by acting on PPAR-gamma receptors.
- Side Effects:
- Increased risk of pathological fractures (especially in women due to decreased bone mineral density)
- Edema (fluid retention, which can lead to weight gain, swelling, and potentially worsen heart failure)
- Weight gain (due to fluid retention and increased fat storage)
- Recurrent dizziness and falls (due to fluid retention causing orthostatic hypotension or worsening heart failure)

9. Insulinoma (Beta Cell Tumor):
- Origin: Arises from the beta cells of the pancreas, leading to excess insulin production.
- Symptoms:
- Hypoglycemia (due to excessive insulin)
- Symptoms like shakiness, sweating, confusion, and loss of consciousness can occur.
- Treatment:
- Octreotide (somatostatin analog) to inhibit insulin release.
- Surgery to remove the tumor.
10. Glucagonoma (Alpha Cell Tumor):
- Origin: Arises from the alpha cells of the pancreas, leading to excess glucagon production.
- Symptoms:
- Declining weight (due to catabolic effects of glucagon)
- Dermatitis: Specifically necrolytic migratory erythema (a characteristic skin rash).
- Depression and diabetes mellitus (due to glucagon-induced hyperglycemia).
- DVT (Deep vein thrombosis) and diarrhea.
- Treatment:
- Octreotide to suppress glucagon secretion.
- Surgery to remove the tumor.
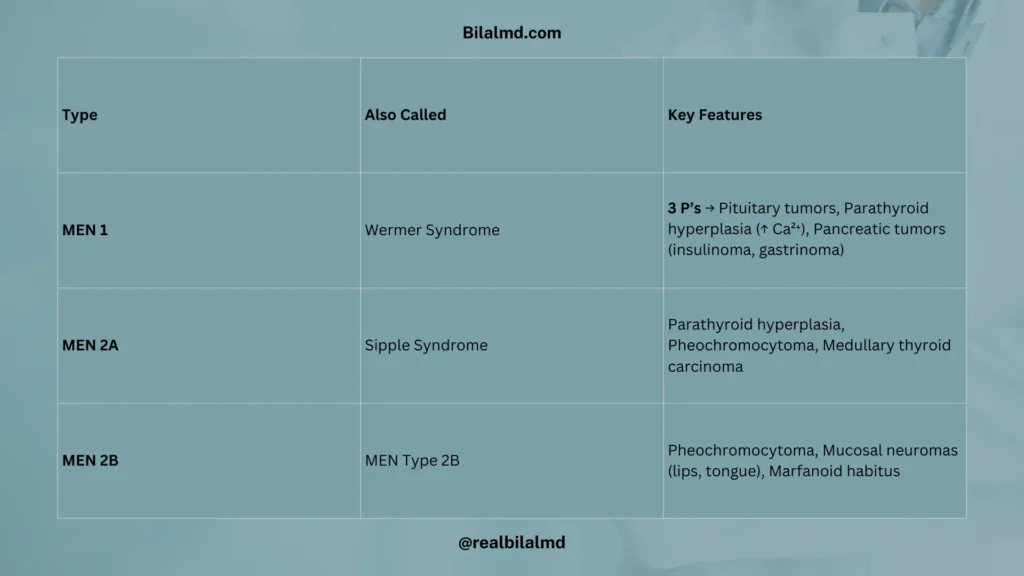
11. Multiple Endocrine Neoplasia (MEN)
There are 3 types of Multiple Endocrine Neoplasia (MEN), each with specific characteristics:
- MEN Type 1 (Wermer Syndrome)
- MEN Type 2A (Sipple Syndrome)
- MEN Type 2B (Multiple Endocrine Neoplasia Type 2B)
1. MEN Type 1 (Wermer Syndrome):
- Key Features:
- Pituitary tumors (e.g., prolactinomas)
- Parathyroid hyperplasia (leading to hypercalcemia)
- Pancreatic tumors (e.g., insulinomas, gastrinomas)
2. MEN Type 2A (Sipple Syndrome):
- Key Features:
- Parathyroid hyperplasia (hypercalcemia)
- Pheochromocytomas (tumors of the adrenal glands producing catecholamines)
- Medullary Cancer (carcinoma of the thyroid)
3. MEN Type 2B:
- Key Features:
- Pheochromocytomas (adrenal tumors)
- Mucosal neuromas (benign tumors affecting mucosal surfaces, like lips and tongue)
- Marfanoid habitus (tall, thin body with long limbs, similar to Marfan syndrome)
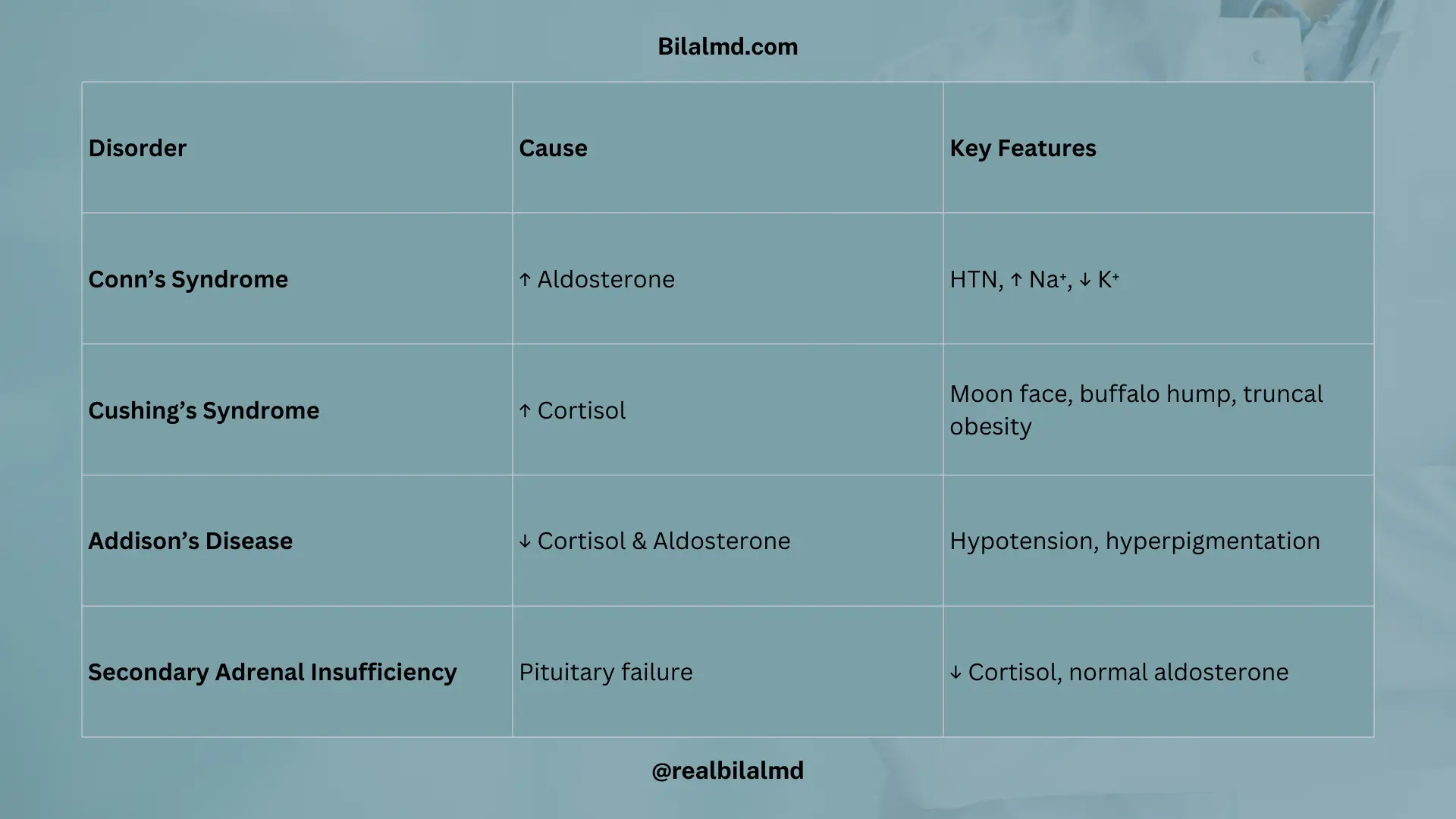
7. Adrenal Gland
Adrenal Gland Structure and Functions:
The adrenal cortex is divided into three parts, each producing a different hormone:
- Zona Reticularis: Produces androgens (influence secondary sexual characteristics).zona glomerulosa – aldosterone
- Zona Glomerulosa: Produces aldosterone (regulates sodium and potassium balance).
- Zona Fasciculata: Produces cortisol (regulates metabolism, immune response).

1. Primary Aldosteronism (Conn’s Syndrome):
- Symptoms:
- History of hypertension (HTN), dizziness, and poor energy.
- Elevated sodium (Na > 145 mEq/L).
- Low potassium (K < 3.5 mEq/L).
- Normal renin levels (primary aldosteronism is often associated with low renin, which further increases aldosterone).
- If renin is also elevated, this leads to secondary hyperaldosteronism. This may occur in conditions like renal artery stenosis, where blood flow to the kidneys is decreased, triggering a compensatory increase in renin, which stimulates aldosterone production.
- Blood volume: In primary aldosteronism, blood volume may decrease, but renin remains low due to the negative feedback loop of elevated aldosterone.
2. Cushing’s Syndrome (Excess Cortisol):
- Symptoms:
- Moon face, buffalo hump, truncal obesity (fat accumulation around the torso, but thin limbs).
- Lab findings: Elevated cortisol levels, but if ACTH is low, cortisol is elevated due to autonomous adrenal production.
- Diagnosis:
- ACTH suppression test: 8 mg high-dose dexamethasone (a synthetic steroid) is administered.
- If ACTH decreases the next morning, the issue is likely pituitary (Cushing’s disease).
- If ACTH increases, it suggests adrenal insufficiency or an adrenal tumor.
- ACTH suppression test: 8 mg high-dose dexamethasone (a synthetic steroid) is administered.
3. Adrenal Insufficiency:
- Primary Adrenal Insufficiency (Addison’s Disease):
- Symptoms:
- Hypoglycemia, dizziness, hypotension, hyperkalemia (due to aldosterone deficiency), low cortisol, low aldosterone, and increased ACTH.
- Pigmented skin (due to increased MSH from ACTH precursor).
- Symptoms:
- Secondary Adrenal Insufficiency (due to pituitary failure, such as from a pituitary tumor):
- Symptoms: Same as primary adrenal insufficiency (hypoglycemia, dizziness, hypotension, etc.).
- Labs: Low cortisol, normal aldosterone, low ACTH (as the pituitary fails to produce ACTH).
- Diagnosis:
- In primary adrenal insufficiency, ACTH levels are elevated due to loss of negative feedback from cortisol.
- Secondary adrenal insufficiency will show low ACTH because the pituitary fails to produce it.
8. Adrenal Medulla
Pheochromocytoma:
- Symptoms:
- Palpitations (due to increased catecholamine release)
- Episodic raised blood pressure (BP) (due to excess catecholamines)
- Headache (due to high blood pressure)
- Increased VMA (Vanillylmandelic acid) in urine (a marker of catecholamine breakdown)
- Mnemonic: 5 P’s of Pheochromocytoma:
- Pressure (high blood pressure)
- Pain in the head (headache)
- Pallor (pale skin, due to vasoconstriction)
- Pain in the limbs (can occur due to vasoconstriction and reduced blood flow)
- Palpitations (heart racing due to excess catecholamines)
- Treatment:
- Phenoxybenzamine: An irreversible alpha blocker that is used to block the effects of excess catecholamines and control blood pressure.
- First step in managing pheochromocytoma before surgery.
- Beta-blockers: After adequate alpha-blockade with phenoxybenzamine, a beta blocker like propranolol is added to control the palpitations and prevent tachycardia.
- Phenoxybenzamine: An irreversible alpha blocker that is used to block the effects of excess catecholamines and control blood pressure.

Check your NRE Step 1 result after completing the exam.